Locations:

Barriers to HPV vaccine utilization

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/3ab6c17e-81ee-4fe2-8998-e569a21226f7/vaccine_650x450_jpg)
vaccine_650x450
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
African American, Hispanic, American Indian and Alaskan Native women continue to be disproportionately affected by cervical cancer compared with white women. From 2006 to 2010, the incidence of cervical cancer in African American women was 10.3 per 100,000; in white women it was 7.2. The mortality rate from cervical cancer in African American women is twice that in white women.
As the first-line healthcare providers for many women, the primary care physician and the general obstetrician-gynecologist are optimally positioned to reduce these disparities. Prevention plays a key role.
Currently, 3 vaccines against HPV are available in the United States, a 2-valent, a 4-valent, and since 2015, a 9-valent preparation.
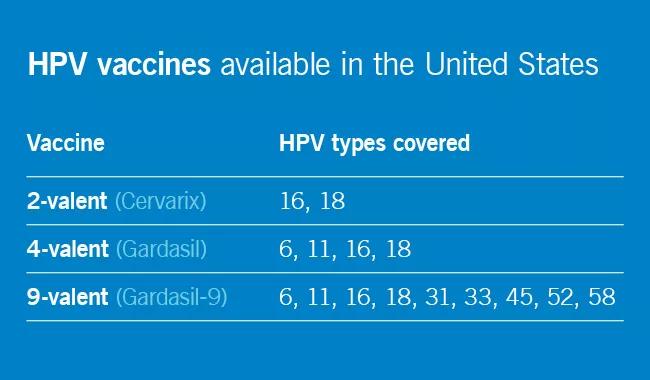
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/4a2f711a-dac7-4ed1-9548-65aa1856fc23/HPV-vaccine_650x380-table_jpg)
The Females United to Unilaterally Reduce Endo/Ectocervical Disease study demonstrated that the 4-valent vaccine was highly effective against cervical intraepithelial neoplasia due to HPV 16 and 18. In another study, the 2-valent vaccine reduced the incidence of CIN 3 or higher by 87 percent in women who received all three doses and who had no evidence of HPV infection at baseline.
HPV vaccination is expensive. Each shot costs about $130, plus the cost of administering it. Although the Vaccines for Children program covers the HPV vaccine for uninsured and underinsured children and adolescents under age 19, Medicaid coverage varies from state to state for adults over age 21.
The Advisory Committee on Immunization Practices (ACIP) recommends routine vaccination for:
Advertisement
In October 2016, the ACIP approved a two-dose series given six to 12 months apart for patients starting vaccination at ages 9 through 14 years who are not immunocompromised. Others should receive a three-dose series, with the second dose given one to two months after the first dose and the third dose given six months after the first dose. Previously, three doses were recommended for everyone.
HPV vaccination rates among adolescents in the United States increased from 33.6 percent in 2013 to 41.7 percent in 2014. However, HPV vaccination rates continue to lag behind those of other routine vaccines, such as Tdap and meningococcal conjugate.
Reagan-Steiner et al reported that more black than white girls age 13 through 17 received at least one dose of a three-dose HPV vaccination series, but more white girls received all three doses (70.6 vs 61.6 percent). In contrast, a meta-analysis by Fisher et al found African American and uninsured women generally less likely to initiate the HPV vaccination series. Kessels et al reported similar findings.
Barriers to HPV vaccination can be provider-dependent, parental, or institutional.
Malo et al surveyed Florida Medicaid providers and found that those who participated in the Vaccines for Children program were less likely to cite lack of reimbursement as a barrier to vaccination.
Meites et al surveyed sexually transmitted disease clinics and found that common reasons for not offering HPV vaccine were cost, staff time and difficulty coordinating follow-up visits to complete the series.
Advertisement
Providers report lack of urgency or lack of perception of cervical cancer as a true public health threat, safety concerns regarding the vaccine and the inability to coadminister vaccines as barriers.
Studies have shown that relatively few parents (up to 18 percent) of parents are concerned about the effect of the vaccine on sexual activity. Rather, they are most likely to cite lack of information regarding the vaccine, lack of physician recommendation and not knowing where to receive the vaccine as barriers.
Guerry et al determined that the single most important factor in vaccine initiation was physician recommendation, a finding reiterated in other studies. A study in North Carolina identified failure of physician recommendation as one of the missed opportunities for vaccination of young women.
Therefore, the primary care physician, as the initial contact with the child or young adult, holds a responsibility to narrow this gap. In simply discussing and recommending the vaccine, physicians could increase vaccination rates.
Dr. Mahdi is a gynecologic oncologist at Cleveland Clinic.
This is an abridged excerpt from an article previously printed in Cleveland Clinic Journal of Medicine. For full article, author and reference lists, click here.
Advertisement
Advertisement

First-of-its-kind research investigates the viability of standard screening to reduce the burden of late-stage cancer diagnoses

Global R&D efforts expanding first-line and relapse therapy options for patients

Study demonstrates ability to reduce patients’ reliance on phlebotomies to stabilize hematocrit levels

A case study on the value of access to novel therapies through clinical trials

Findings highlight an association between obesity and an increased incidence of moderate-severe disease

Cleveland Clinic Cancer Institute takes multi-faceted approach to increasing clinical trial access 23456

Key learnings from DESTINY trials

Overall survival in patients treated since 2008 is nearly 20% higher than in earlier patients