Locations:

Procedure has potential benefits but entails teamwork

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/469fdd0e-4566-4169-b2f7-3ef9e29495d1/15-URL-3019-Ramirez-Haber-Hero-Image_jpg)
15-URL-3019-Ramirez-Haber-Hero-Image
By Daniel Ramirez, MD, and Georges-Pascal Haber, MD, PhD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Renal cell carcinoma (RCC) rarely occurs in women of childbearing age, with an estimated annual incidence of less than five cases per 100,000 women. Nevertheless, renal surgery during pregnancy may be necessary for management of large tumors, lesions at risk for hemorrhage, or active bleeding. Such surgery has previously been shown to be feasible when indicated.
Laparoscopic surgery offers many advantages over open surgery for management of renal neoplasms in the pregnant patient, including decreased rates of wound complications, decreased risk of maternal hypoventilation, decreased risk of respiratory depression in the fetus in light of reduced narcotic requirement for postoperative pain control, and shorter hospitalization with faster convalescence.
Only a handful of reports of laparoscopic nephrectomy during pregnancy have been described in the literature. Historically, surgical procedures were postponed until the second trimester of pregnancy to avoid the danger of spontaneous abortion during the first trimester or preterm labor during the third trimester, but contemporary studies and guidelines report that surgical procedures may be safely performed at any time during pregnancy.
While the literature does not currently address the use of the robotic platform for performing laparoscopic procedures in these circumstances, the same surgical tenets exist for this approach.
Our institution recently performed the first reported robotic partial nephrectomy in a 35-year-old healthy pregnant patient at 20 weeks gestation for treatment of a 7.5 cm renal mass with a RENAL score of 11.
Advertisement
Diagnosis of the mass was made during routine anatomical ultrasonography of the fetus at 18 weeks gestation. The patient ultimately underwent MRI with gadolinium contrast to better characterize the mass (Figure 1). On MRI she was found to have an enhancing 7.5 cm right-sided upper pole renal mass, consistent with RCC.
Figure 1. MRI scan shows a 7.5 cm right-sided renal mass in a pregnant patient at 20 weeks gestation.
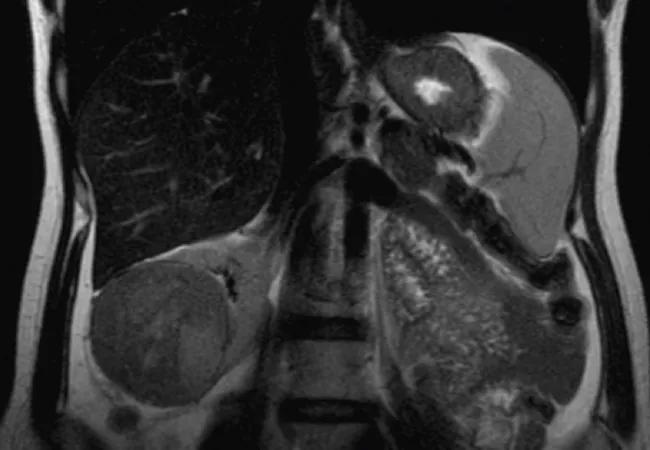
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/98a2d585-e7c6-4547-8aa8-16162ea513c7/15-URL-3019-Ramirez-Haber-Inset-Image-01_jpg)
A. Coronal view
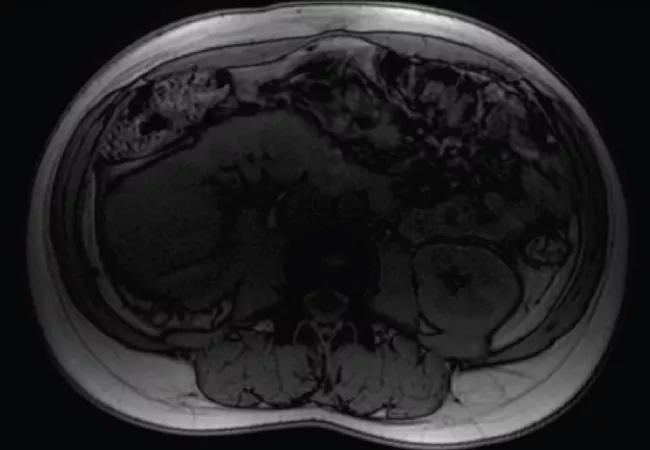
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/3bc44cb0-ad2d-4829-8c94-a2980046d597/15-URL-3019-Ramirez-Haber-Inset-Image-02_jpg)
B. Axial view
Perioperatively, her case was managed using a multidisciplinary approach, with cooperation among specialists in anesthesia, high-risk obstetrics, maternal fetal medicine, urology and our institutional bioethics committee. After a thorough discussion about the potential risks and benefits of surveillance until after delivery, renal mass biopsy and surgery, the patient and her family decided to proceed with robotic partial nephrectomy. Preoperatively the patient’s serum creatinine was 0.54 mg/dL and her hemoglobin was 11.2 g/dL.
Intraoperatively, the patient was placed in left lateral decubitus position, with her right side up. Fortunately, she presented with a right-sided renal neoplasm, allowing for left lateral decubitus positioning. In this position, the gravid uterus falls away from the inferior vena cava (IVC), reducing the IVC’s compression. Compression of the IVC may considerably reduce venous return to the heart, resulting in diminished cardiac output and potential maternal hypotension, with possible decreased placental and fetal perfusion during surgery.
Advertisement
Intra-abdominal access was obtained with the Veress needle lateral to the lateral border of the rectus muscle at the level of the 11th rib. This access was obtained more lateral to where we usually obtain access in order to avoid the gravid uterus. Contemporary guidelines suggest that laparoscopic access during pregnancy may be performed via an open Hasson technique, optical trocar, or use of Veress needle with modification of location depending on prior surgery and fundal height. Insufflation was maintained at or below 12 mmHg to decrease the risk of IVC or pulmonary compression, since pregnant women experience reduced lung pulmonary volumes and lower functional residual capacity secondary to diaphragmatic displacement from a gravid uterus.
Operative time was 253 minutes, warm ischemia time was 36 minutes, and estimated blood loss was 120 mL. The patient had a routine post-operative course and recovered well. Prophylactic heparin was avoided to decrease the risk of bleeding after partial nephrectomy.
Maternal fetal medicine and obstetrics assessed the patient and fetus prior to surgery, immediately after surgery in the post-anesthesia care unit, and daily during her hospitalization and found normal fetal movements and heart tones at each evaluation. The patient’s creatinine peaked at 0.81 mg/dL and her hemoglobin reached a nadir of 9.6 g/dL. She was discharged on postoperative day six in excellent condition. Final pathology demonstrated a 6.6 cm chromophobe renal cell carcinoma with negative margins.
Advertisement
Four months later, the patient vaginally delivered her baby boy at term without complications.
We found that robotic partial nephrectomy during pregnancy is safe and feasible but requires multidisciplinary cooperation and careful operative planning to ensure optimal safety of mother and fetus. Early involvement of high-risk maternal fetal medicine, obstetrics, anesthesiology and pharmacy are imperative to ensure optimal outcomes.
Dr. Ramirez is a clinical fellow in Cleveland Clinic Glickman Urological & Kidney Institute’s Department of Urology. Dr. Haber is a staff member of the Department of Urology.
Advertisement
Advertisement

First-of-its-kind research investigates the viability of standard screening to reduce the burden of late-stage cancer diagnoses

Global R&D efforts expanding first-line and relapse therapy options for patients

Study demonstrates ability to reduce patients’ reliance on phlebotomies to stabilize hematocrit levels

A case study on the value of access to novel therapies through clinical trials

Findings highlight an association between obesity and an increased incidence of moderate-severe disease

Cleveland Clinic Cancer Institute takes multi-faceted approach to increasing clinical trial access 23456

Key learnings from DESTINY trials

Overall survival in patients treated since 2008 is nearly 20% higher than in earlier patients