Locations:

Unrecognized cases lead to incomplete excisions

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/8a7a363b-8ff5-466a-99dc-b9b9d7dcd808/14-ORT-1692-Mesko-Hero-Image-690x380pxl_jpg)
14-ORT-1692-Mesko-Hero-Image-690x380pxl
By Nathan W. Mesko, MD, Michael J. Joyce, MD, and Steven A. Lietman, MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
noun \ze-br , Canada & British also ze-\
Sarcoma represents a rare form of malignancy, accounting for 1 percent of all adult malignancy diagnoses. Despite long-standing educational efforts to increase recognition and improve practice patterns surrounding sarcoma care, the literature shows persistently high rates (19 to 60 percent) of unrecognized soft tissue sarcomas that undergo inappropriate, margin-positive surgical excision. This troubling trend endures in spite of clear guidelines that help highlight those new “lumps and bumps” that should be considered high risk for a potential sarcoma diagnosis.1,2 Efforts to curb this trend continue, with the goal of early referral of patients with suspicious soft tissue masses to an orthopaedic oncologist to enhance the opportunity for a successful outcome.
Literature suggests that the average primary care physician or non-sarcoma-trained surgeon encounters a true sarcoma diagnosis only once or twice in his or her career. The American Cancer Society projected that about 12,000 new soft tissue sarcoma diagnoses would be made in 2014.3 This represents only 5 percent of the projected new diagnoses of cancers of the breast, prostate or lung, which helps explain why only a handful of U.S. medical centers have the resources needed to treat and follow patients with a new sarcoma diagnosis effectively. Moreover, it is well established that definitive care administered at high-volume institutions with a functioning multidisciplinary sarcoma team leads to lower complication and mortality rates and better functional outcomes.4
Advertisement
Unrecognized soft tissue sarcomas can be problematic for two main reasons:

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/8a7a363b-8ff5-466a-99dc-b9b9d7dcd808/14-ORT-1692-Mesko-Hero-Image-690x380pxl_jpg)
Figure. Photos from a case illustrating the consequences of incomplete excision. Left panel: A middle-aged man presented to clinic following excision of a “benign lipoma” at an outside institution. The excision was done through a 10-cm transverse incision over the posterolateral aspect of the left thigh, with a drain placed 3 cm distal to the incision. No preoperative imaging was obtained. Pathology was consistent with a high-grade soft tissue sarcoma. Right panel: In the OR, the incision was marked out to provide no less than 2 cm of skin surrounding the incision, as carefully correlated with a preoperative MRI. The wound ultimately required split-thickness skin graft coverage to achieve closure.
Advertisement
For physicians, maintaining proper suspicion for such a rare entity can be difficult. In collaboration with Vanderbilt University’s sarcoma team, Dr. Mesko looked at inciting causes for litigation surrounding sarcoma care since 1980,5 with the goal of better describing risk factors for litigation to help improve education. Key findings (Table) included:
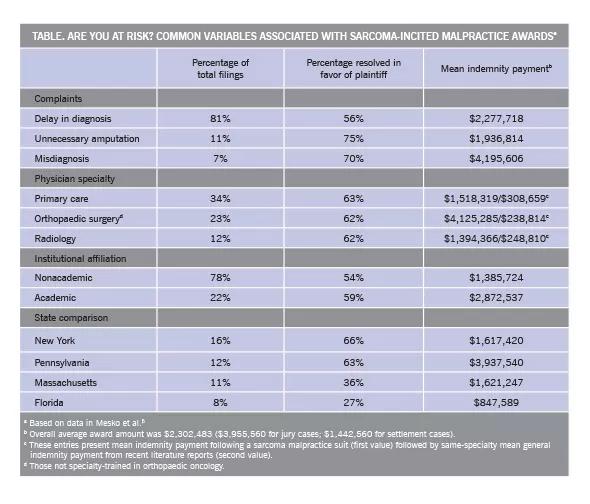
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/eedb34a2-c705-48d7-95ef-7654455538fe/14-ORT-1692-Mesko-Inset-Image-Table-590pxl-width_jpg)
The overall study revealed that while sarcomas are rare, the ramifications of incorrectly identifying and treating a potential sarcoma can be very real to both physician and patient.
Cleveland Clinic houses a multidisciplinary sarcoma team that comprises multiple physician specialties and has a singular purpose of providing the care and resources to bring about the best possible patient outcome. In addition to our staff of orthopaedic oncologists, this team includes radiation oncologists with special interests in pre-, intra- and postoperative radiation therapy; pathology specialists with expertise in soft tissue sarcoma who minimize chances of a misdiagnosis; and medical oncologists who have deep experience in evaluating the role of adjuvant medical therapy for these rare malignancies. We believe firmly in collaboration with other institutions with specialized sarcoma expertise to answer questions that will push the envelope for sarcoma treatments in the future.
Advertisement
Because sarcoma is a rare entity, any lesion that arouses suspicion for a potential sarcoma diagnosis should have a low threshold for referral to a facility with an orthopaedic oncologist who works as part of a multidisciplinary sarcoma team. Together, with proper sarcoma awareness, we can begin to change these troubling patterns of delayed diagnosis and improper excision surrounding this rare “zebra” diagnosis.
Dr. Mesko is an orthopaedic oncologist with Cleveland Clinic’s Musculoskeletal Tumor Center in the Department of Orthopaedic Surgery.
Advertisement
Advertisement

First-of-its-kind research investigates the viability of standard screening to reduce the burden of late-stage cancer diagnoses

Global R&D efforts expanding first-line and relapse therapy options for patients

Study demonstrates ability to reduce patients’ reliance on phlebotomies to stabilize hematocrit levels

A case study on the value of access to novel therapies through clinical trials

Findings highlight an association between obesity and an increased incidence of moderate-severe disease

Cleveland Clinic Cancer Institute takes multi-faceted approach to increasing clinical trial access 23456

Key learnings from DESTINY trials

Overall survival in patients treated since 2008 is nearly 20% higher than in earlier patients