Locations:

Review of common hereditary syndromes

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/a82a2843-e3ee-44e7-969c-a270a93f2a13/Breast-cancer_650x450_jpg)
Breast-cancer_650x450
By Holly J. Pederson, MD, and Stephen Grobmyer, MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
While most cases of breast cancer are sporadic, up to 10 percent are attributable to single-gene hereditary cancer syndromes. People with these syndromes have a lifetime risk of breast cancer much higher than in the general population, and the cancers often occur at a much earlier age.
With genetic testing becoming more common, primary care physicians need to be familiar with the known syndromes, associated risks and evidence-based recommendations for management.
Women who have a hereditary predisposition to breast cancer face complex and emotional decisions about the best ways to manage and reduce their risks. Their management includes close clinical surveillance, chemoprevention and surgical risk reduction.
Referral to multiple subspecialists is an important component of these patients’ preventive care. They may need referrals to a cancer genetic counselor, a high-risk breast clinic, a gynecologic oncologist and counseling services. They may also require referrals to gastroenterologists, colorectal surgeons, endocrinologists and endocrine surgeons, depending on the syndrome identified.
Screening and management guidelines for hereditary breast cancer syndromes are evolving. While subspecialists may be involved in enhanced surveillance and preventive care, the primary care physician is the central player, with both a broader perspective and knowledge of the patient’s competing medical issues, risks and preferences.
In addition to breast cancer, the risk of other malignancies is also higher, with the pattern varying by syndrome. Primary care physicians need to be familiar with these risks to provide adequate referrals.
Advertisement
Even without a hereditary cancer syndrome, a combination of reproductive, environmental, personal and family history factors can confer a 20 percent lifetime risk. But for women with hereditary syndromes, the risk far exceeds 20 percent regardless of such risk factors.
In general, referral for genetic counseling should be considered for patients and their families who have:
The most common hereditary breast cancers and their incidences and risks are listed in the below table.
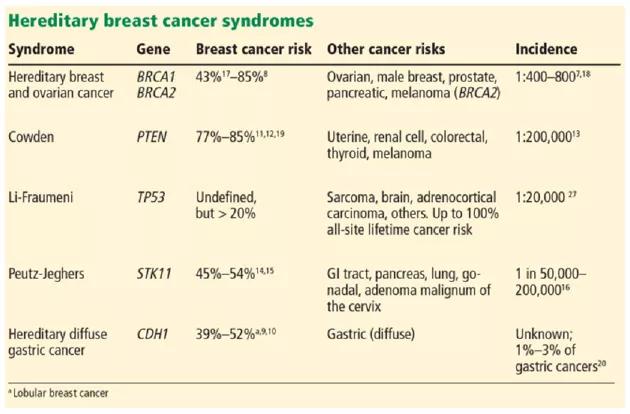
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/020c5401-d43e-479f-898b-32c0471b8ea1/Table-1_630x414_jpg)
Management for patients at high risk falls into three broad categories: clinical surveillance, chemoprevention and surgical risk reduction. The utility and benefit of each depend to a large degree on the patient’s specific mutation, family history and comorbidities. Decisions must be shared with the patient.
Close clinical surveillance
Consensus guidelines for cancer screening in the syndromes described here are summarized in the table below. While the guidelines are broadly applicable to all women with these conditions, some individualization is required based on personal and family medical history.
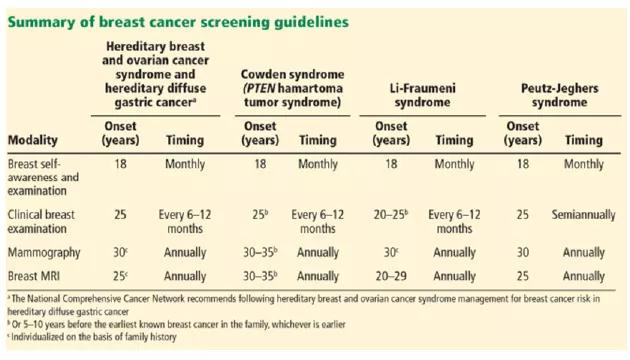
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/e404eebe-11b9-4822-876c-7f09b4890cf8/Table-2_630x360_jpg)
In general, screening begins at the ages listed above or 10 years earlier than the age at which cancer developed in the first affected relative, whichever is earlier.
Advertisement
Chemoprevention
Certain selective estrogen receptor modulators and aromatase inhibitors decrease the risk of invasive breast cancer in healthy women at high risk. These drugs include tamoxifen, which can be used before menopause, and raloxifene, anastrozole and exemestane, which must be used only after menopause.
Because data are limited, we cannot make any generalized recommendations about chemoprevention in patients with hereditary breast cancer syndromes. Decisions about chemoprevention should take into account the patient’s personal and family histories. Often, a medical oncologist or medical breast specialist can help by discussing the risks and benefits for the individual patient.
Surgical prophylaxis
Surgical prophylactic options for patients at genetic risk of breast cancer are bilateral mastectomy and bilateral salpingo-oophorectomy.
Bilateral risk-reducing mastectomy reduces the risk of breast cancer by at least 90 percent and greatly reduces the need for complex surveillance. In patients at very high risk of breast cancer, risk-reducing operations also reduce the risk of ultimately needing chemotherapy and radiation to treat breast cancer.
The timing of risk-reducing mastectomy depends largely on personal and family medical history and personal choice. Bilateral mastectomy at age 25 results in the greatest survival gain for patients with hereditary breast and ovarian cancer syndrome. Such precise data are not available for other hereditary cancer syndromes, but it is reasonable to consider bilateral mastectomy as an option for any woman with a highly penetrant genetic mutation that predisposes her to breast cancer. Special consideration in the timing of risk-reducing mastectomy must be given to women with Li-Fraumeni syndrome, as this condition is often associated with an earlier age at breast cancer diagnosis (before age 30).
Advertisement
In patients who have pathogenic mutations in BRCA1 or 2, prophylactic salpingo-oophorectomy is the only intervention that has been shown to reduce mortality. We recommend that women with hereditary breast and ovarian cancer syndrome strongly consider prophylactic salpingo-oophorectomy by age 40 or when childbearing is complete for the greatest reduction in risk.
Dr. Pederson directs Medical Breast Services in the Comprehensive Breast Cancer Program at Cleveland Clinic Cancer Center. Dr. Grobmyer co-directs the Program.
This article originally appeared in Cleveland Clinic Journal of Medicine and has been edited for length. For the full article and reference list, visit Cleveland Clinic Journal of Medicine.
Advertisement
Advertisement

First-of-its-kind research investigates the viability of standard screening to reduce the burden of late-stage cancer diagnoses

Global R&D efforts expanding first-line and relapse therapy options for patients

Study demonstrates ability to reduce patients’ reliance on phlebotomies to stabilize hematocrit levels

A case study on the value of access to novel therapies through clinical trials

Findings highlight an association between obesity and an increased incidence of moderate-severe disease

Cleveland Clinic Cancer Institute takes multi-faceted approach to increasing clinical trial access 23456

Key learnings from DESTINY trials

Overall survival in patients treated since 2008 is nearly 20% higher than in earlier patients