Locations:

Collaboration between centers helps ability to breathe

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/eb41d232-6f6d-47e0-a42e-0c3aaa7cf672/14-ENT-2024-MIlstein-Hero-Image-690x380pxl_jpg)
14-ENT-2024-MIlstein-Hero-Image-690x380pxl
By Claudio F. Milstein, PhD, and Douglas M. Hicks, PhD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Patients with laryngeal hyper-responsiveness (LHR) who come to Cleveland Clinic for care are the beneficiaries of a fruitful clinical alliance between the Voice Center in the Head & Neck Institute and the Asthma Center in the Respiratory Institute.
Specialists in these two areas have joined forces to provide more effective care for LHR patients, whose constellation of symptoms can defy easy diagnosis. These symptoms can include, among others:
In some patients with LHR, relentless symptoms persist for years, even decades, and frequent hospitalizations are common. LHR’s impact on daily life is significant, and in some instances it leads to substantial disability.
The collaboration between the Voice Center and the Asthma Center seemed to be a natural response to LHR patients having been referred to both centers for evaluation. These patients often have been misdiagnosed as having asthma or recurrent anaphylaxis, but treatments for these conditions are ineffective and often result in unnecessary medical interventions. The ineffectiveness of care is reflected in a reported mean time to proper diagnosis of 4.5 years.
Among the factors that contribute to the difficulties in establishing a timely diagnosis are a poor understanding of the underlying pathophysiology, the involvement of numerous specialties and a lack of unifying terminology. Fortunately, clinician interest in and understanding of LHR have increased over the past decade, and effective clinical care is reducing the time from symptom onset to proper diagnosis and effective treatment.
Advertisement
There are two keys to managing LHR:
Recent reports of encouraging progress with various neuromodulators (e.g., gabapentin, amitriptyline, tramadol and pregabalin) in some patients further support the idea of CNS involvement.
Once the patient is correctly diagnosed, our prescriptive care goes beyond drug therapy. The efficacy of behavioral therapy has been demonstrated in several randomized trials. Respiratory and laryngeal control therapy, as provided by our expert speech language pathologists, is an essential component of our treatment algorithm.
Because patients who are referred to our centers often travel long distances to be here, efficiency in providing combined care is paramount to offering them the best overall experience. For example, regardless of where patients with possible LHR enter our system, they are scheduled to be seen at both the Voice Center and the Asthma Center. The degree of cooperation between our centers is uncommon at many other major healthcare facilities, and we encourage voice specialists at all levels to reach out to colleagues in pulmonary and allergy medicine to develop a similar collaboration.
Advertisement
Establishing a professional network with other specialists, with fluid communication among providers, and providing easy access for patients are the keys to providing state-of-the-art care for patients with respiratory disorders of laryngeal etiology.
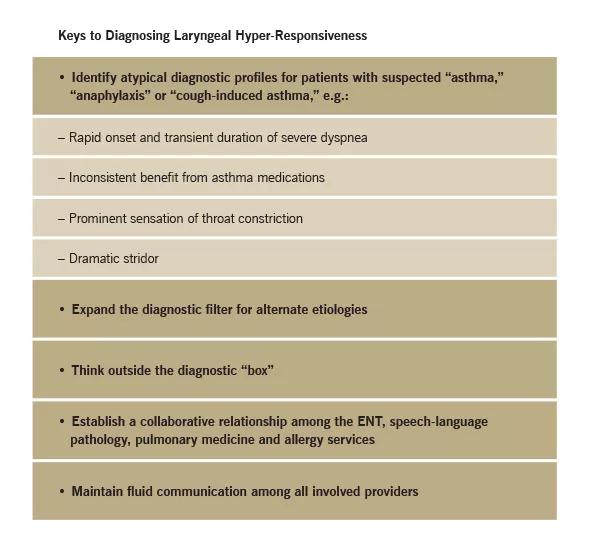
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/9ad9c078-a759-4e97-bf14-368023e68981/14-ENT-2023-Milstein-Inset-Image-Table-590pxl-width_jpg)
Dr. Milstein is Director of the Voice Center and Section-Head, Division of Speech Language Pathology
Advertisement
Advertisement

With a wide scope of skills, comprehensive otolaryngologists care for patients of all ages in the community

Research on children with UHL explores the quality-of-life benefits and outcomes of cochlear implants

A look at how custom-fitted oral appliances work and when they’re a good fit for patients
Subtle information gleaned from clinical examinations prompted concern

A new single-port system well-suited for oropharyngeal cancer treatment

Challenging case requires outside-the-box approach

Collaborative and multidisciplinary approach necessary for treatment

The tri-vector gracilis procedure uses a thin muscle from the thigh to help create a natural mimetic smile