Locations:

Weighing risks and benefits of radiation-based imaging modalities

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/c7c95d04-a41f-4793-9639-45c42819c8b1/16-PUL-2404-Krishnan-Hero-Image-650x450pxl_jpg)
16-pul-2404-krishnan-hero-image-650x450pxl
By Sudhir Krishnan, MD, and Jorge Guzman, MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Critically ill patients admitted to a MICU are often subjected to multiple radiation-based diagnostic studies. The past decade has seen a dramatic rise in the utilization of radiation-based imaging studies, interventional procedures and computed tomography (CT). Medical radiation now accounts for a significant proportion of all radiation exposure in the United States. This has led to increased scrutiny of the stochastic effects (probability of cancer induction) of radiation and the subsequent risk of cancer induction.
In an effort to quantify and characterize medical radiation exposure in the MICU, we conducted a study to examine the radiation burden per episode of care in a cohort of patients admitted to the MICU at Cleveland Clinic’s main campus. We found significant levels of exposure in some patients.
To quantify radiation burden in the MICU, our study collated and summated radiation doses from all radiographic studies to arrive at a cumulative effective dose (CED) in millisieverts (mSv).
The absorbed dose (energy deposited by ionizing radiation in biological tissues) is converted into an effective dose by correcting for both the type of radiation used (e.g., gamma versus x-rays) and a weighting factor for the tissue or organ being irradiated. The effective dose calculation allows for summation of doses from all sources of radiation and represents the stochastic effect of low levels of ionizing radiation.
Eighty-four percent of the 4,155 admissions (3,333 unique patients) to the MICU in 2013 were exposed to at least one imaging study. Approximately 2.3 percent (N = 98) of MICU admissions were exposed to a CED greater than the annual federal occupational limit (50 mSv). Twelve admissions (nine MICU survivors) were exposed to doses greater than 100 mSv, similar to those accrued by some Japanese survivors of the atomic bomb blasts in 1945. This dosage is statistically linked with cancer induction.
Advertisement
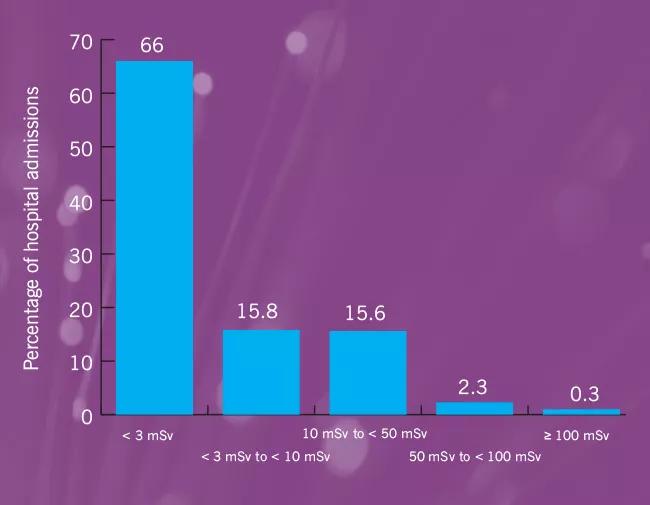
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/4e8ebb93-672e-4326-b675-8368e0011f2a/16-PUL-2404-Krishnan-Inset-Image-01-650pxl-width_jpg)
Figure 1: Overall distribution of cumulative effective dose (CED) of radiation in the study population.
Fifty-seven percent of the total radiation dose exposure came from CT scans.
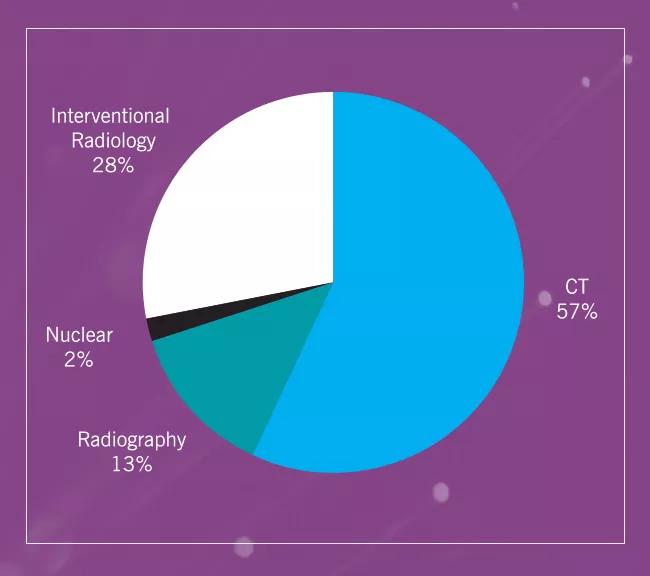
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/387a66aa-b400-4968-a0cb-9419c0d3aa31/16-PUL-2404-Krishnan-Inset-Image-02-650pxl-width_jpg)
Figure 2: Distribution of average CED per episode of care in the MICU by type of radiological study.
The diagnostic utility of radiation imaging in the care of the critically ill should not be understated. However, patients in the MICU may be inadvertently exposed to very high dosages of radiation, due to the lack of a dose-tracking system. The risk of exposing patients to increasing radiation doses and the theoretical lifetime risk of cancer induction must be weighed against the purported benefits of further testing.
The proportion of patients exposed to radiation doses in excess of 50 mSV would increase dramatically if one were to collate the radiation burden acquired annually over the course of continued clinical care.
Focusing on statistical risks from radiation imaging should not distract attention from the potential benefits of imaging studies. Effective and judicious utilization of radiological resources provides great benefit to those needing diagnostic imaging studies. In the absence of a local, regional or national authority to monitor the cumulative doses accrued by patients, the requesting physician must be a responsible and economical consumer of radiological resources.
In our ongoing effort to quantify and explore radiation exposure in the critically ill, we are examining the annual radiation burden accrued by young patients (< 40 years of age) who survived an episode of critical illness in the MICU. Medical radiation doses accrued as a result of ongoing clinical care from various radiographic modalities both in inpatient and outpatient clinical settings, before and after MICU admission, will be summated to arrive at an annual CED. We hope to partner with other healthcare systems in our region to compare our practices and resulting radiation burden per episode of MICU care.
Advertisement
We ultimately hope to develop a software tool that tracks radiation doses and maintains a registry of radiation accrued per episode of clinical care, year and lifetime. Such a longitudinal registry would benefit clinical research and allow the requesting physician and patient to make an informed choice.
Dr. Krishnan is staff in Critical Care Medicine and Pulmonary Medicine.
Dr. Guzman is Chief Medical Officer, Cleveland Clinic Abu Dhabi.
Advertisement
Advertisement

Volatile organic compounds have potential in heart failure diagnostics

Caregivers are provided with real-time bronchoscopy patient findings

Insights for diagnosing, assessing and treating

A Cleveland Clinic pulmonologist highlights several factors to be aware of when treating patients

New program sets out to better support underserved patient populations

Cleveland Clinic pulmonologists aim to further lower waitlist times and patient mortality

Lessons learned from cohorting patients and standardizing care

New tools and protocols to improve care