Locations:

Harnessing the capacity for plasticity to boost outcomes

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/12ea4fac-8a85-4259-9a9b-72868379773e/plow-690x380_jpg)
plow-690×380
By Ela Plow, PhD, PT; Kelsey Potter-Baker, PhD; and Patrick Chabra, BS
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Injury to the spinal cord (SCI) remains one of the most common and debilitating causes of long-term disability among young adults, particularly war veterans. With approximately 11,000 new cases every year, the prevalence of SCI has exceeded 253,000 cases in just the United States.
Unfortunately, the costs related to SCI management are rising along with the injury’s prevalence. Estimated annual medical care and living expenses, without accounting for indirect costs such as lost wages and productivity, ranged from $67,415 to $181,328 per patient in 2013. This situation is further compounded by evidence that SCI primarily affects younger adults, ultimately resulting in a serious economic, social and personal burden.
The goal of a Department of Defense-funded clinical trial we are conducting is to maximize the recovery potential in adults with SCI using a cost-effective and minimally invasive strategy. Within our trial, we focus on patients with quadriplegia from an injury to the cervical spinal cord, paralyzing not only the lower extremities and trunk but the upper limbs. We have chosen to emphasize recovery in quadriplegia because it imposes significantly greater healthcare costs compared with paraplegia. Further, it has been reported that 75 percent of quadriplegic patients would prefer to have their upper limb function restored more than any other deficit.
An optimistic view of SCI is that the majority of injuries are incomplete. Specifically, in more than 65 percent of patients, injury results in varying degrees of upper extremity deficit. This suggests that many patients with SCI have an ability to transmit information from the brain to affected muscles through spared, albeit fragmented, neural networks. In addition, when one considers that an injury that damages the spinal cord often spares the brain, the advantage of an incomplete injury becomes even more powerful. Our viewpoint becomes clearer below.
Advertisement
The brain, especially its regions such as the motor cortex devoted to upper limb movement, has an extraordinary capacity for fast-paced plasticity. In the context of SCI, brain plasticity can be both beneficial and detrimental.
As SCI patients increasingly use their spared muscles at the cost of paralyzed ones, motor cortical memory of paralyzed muscles decreases. The cortex begins to lose the memory of paralyzed muscles and limbs caudal to the lesion, while magnifying representations of the more spared segments, thus often overtaking territories previously occupied by the now paralyzed muscles.
This maladaptive biological response can hinder rehabilitative efforts. Mainly, since rehabilitation often emphasizes greater use of the more affected muscles, a possible loss of paralyzed muscle cortical representations in the brain can make successful rehabilitation an arduous process.
In our clinical trial, we aim to harness the brain’s fast-paced capacity to exhibit plasticity. Specifically, we intend to take advantage of the fact that the brain can still transmit information, albeit partially, via fragmented but spared pathways to affected muscles.
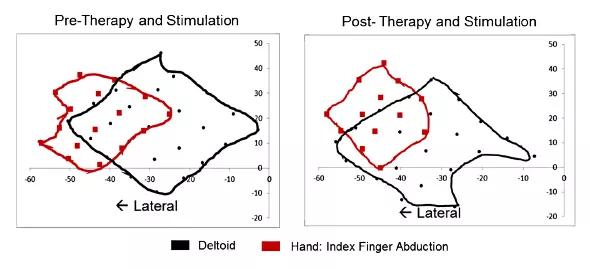
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/c3ab14dd-6899-44be-806e-63c04b72d2a3/plow-fig-1_jpg)
FIGURE 1. Enhanced brain plasticity following stimulation results in the augmentation of spared (red) muscle cortical regions.Enhanced brain plasticity following stimulation results in the augmentation of spared (red) muscle cortical regions.
To do this, we first identify the brain’s existing representations of muscles so that we can understand how territories previously occupied by now paralyzed muscles have been compromised. A neurophysiologic technique called transcranial magnetic stimulation (TMS) is a powerful tool to generate such assessments (see Figure 2A, where representations are being mapped with TMS). With these maps, we can determine the spread of representations of muscles in the brain, while with white matter imaging we can view the pathways they project to the spinal cord (Figure 2B).
Advertisement
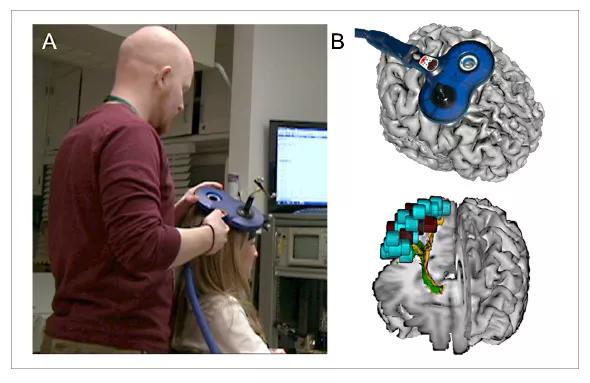
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/e88437c2-408e-4510-bd2a-a3c9729f9440/plow-fig-2_jpg)
FIGURE 2. (A) Stereotactically guided transcranial magnetic stimulation is used to identify muscle cortical regions. (B) White matter imaging shows the muscle cortical regions’ projections to the spinal cord.
Once these representations are mapped with TMS and imaging, we apply facilitatory transcranial direct current stimulation (tDCS) to these regions devoted to the weaker muscles while patients take part in extensive rehabilitation exercises. In doing so, we aim to promote neuronal excitability and restore cortical representations of the paralyzed muscle regions. tDCS uses electrodes placed on the scalp to deliver low levels of direct current that modify cortical excitability. Patients in the experimental group of our study receive one hour of tDCS per day for 10 days in conjunction with rehabilitation sessions.
The process of delivering stimulation during rehabilitation augments the efficacy of rehabilitation. While the brain may not be the source of deficit in SCI, we propose that cortical hindrance to rehabilitation, when removed by stimulation of the paralyzed muscle cortical regions, can result in underrepresented muscles serving as a powerful catalyst for recovery.
To gain maximum adjunctive advantage, in our study we stimulate the cortical regions of the paralyzed muscle during rehabilitation, which ensures that plasticity of weak cortical networks is augmented and that the cost-effectiveness of delivering treatments is improved.
To assess the effectiveness of tDCS in directing neuroplasticity to improve rehabilitative outcomes, we measure study participants’ upper limb function at several time points and compare to baseline to determine if any changes have occurred. We also perform repeat mapping with TMS to understand whether representations of paralyzed muscles are re-established in the brain’s cortical regions.
Advertisement
Patient safety is an important consideration when applying brain stimulation. The noninvasive nature of tDCS, which employs extracephalic electrodes, provides a margin of safety. Currents delivered to the scalp are low, ranging from 1 to 2 mA, and since they are delivered via large electrodes (25 to 35 cm2) in saline-soaked sponges, they are not perceived as uncomfortable. Some patients with SCI, however, present with contraindications to brain stimulation procedures. Contraindications may include history of seizures and/or use of medications that may affect a patient’s threshold for seizures.
Recruiting medically stable patients who are able to travel to Cleveland Clinic to receive intensive rehabilitation and brain stimulation can be challenging. Our recruitment efforts are strongly supplemented by Cleveland Clinic’s Knowledge Program, a health information data collection system that includes information obtained from patients via electronic questionnaires as well as clinical data extracted from Cleveland Clinic’s electronic medical record.
The Knowledge Program logs each neurological outpatient visit, providing valuable long-term and follow-up information and aiding study recruitment. We also have been able to develop pools of candidates using other electronic databases, patient support groups, national foundations and organizations such as Paralyzed Veterans of America and the United Spinal Association.
In sum, with the use of low-cost modalities such as noninvasive brain stimulation and resource-effective strategies such as rehabilitation, we aim to mitigate the economic burden of SCI. Since we target one of the most viable and plastic substrates in patient recovery ‒ motor cortices of the brain ‒ we believe we will be able to harness the potential of incomplete injuries to the spinal cord to maximize improvements to patients’ quality of life.
Advertisement
Dr. Plow is an assistant staff member in Cleveland Clinic Lerner Research Institute’s Department of Biomedical Engineering. Dr. Potter-Baker, a postdoctoral fellow at Lerner Research Institute, and Mr. Chabra, a medical student, are working on the tDCS clinical trial.
Advertisement

New study advances understanding of patient-defined goals

Testing options and therapies are expanding for this poorly understood sleep disorder

Real-world claims data and tissue culture studies set the stage for randomized clinical testing

Digital subtraction angiography remains central to assessment of ‘benign’ PMSAH

Cleveland Clinic neuromuscular specialist shares insights on AI in his field and beyond

Findings challenge dogma that microglia are exclusively destructive regardless of location in brain

Neurology is especially well positioned for opportunities to enhance clinical care and medical training

New review distills insights from studies over the past decade