Locations:

Why ultrasound is ideal for injection guidance in kids
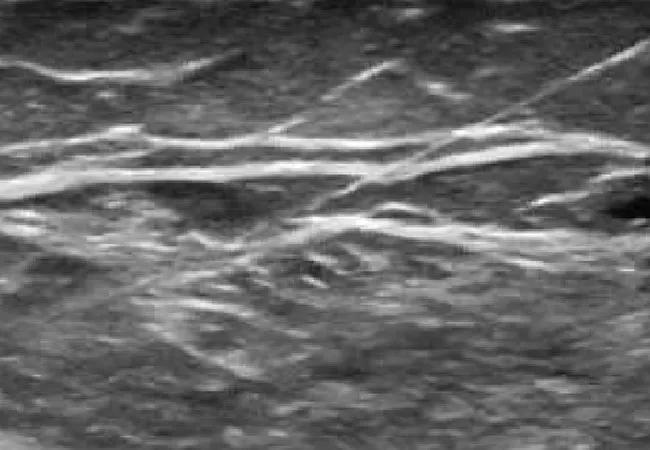
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/1ae48575-81f5-43b3-af48-5f9fee3e3b3e/15-NEU-2527-Aldosari-650x450_jpg)
15-NEU-2527-Aldosari-650×450
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Botulinum neurotoxin (BoNT) selectively blocks the release of acetylcholine at the cholinergic nerve terminal, causing temporary, focal chemodenervation of muscles and resultant reduction in spasticity.
When Koman and colleagues published results of the first clinical trial of BoNT for spasticity in patients with cerebral palsy, their rationale for using BoNT was that spasticity reduction would provide a therapeutic window for intervention and supportive therapies. Since that 1993 publication, BoNT has become widely accepted as a safe and effective option for the treatment of muscle spasticity in the pediatric population.
BoNT treatment is recommended between ages 2 and 6, when gait patterns and motor function are still flexible. When BoNT is used in combination with other modalities, early treatment can delay the need for, and reduce the frequency of, surgical procedures and result in a favorable gait pattern.
Although initial studies focused on BoNT use in ambulatory children with mild impairments, recent studies, including a double-blind, sham-controlled trial, suggested that BoNT can be safe and effective in children with severe cerebral palsy (i.e., gross Motor Function Classification system levels IV and V). Dystonia, excessive drooling and tics are examples of other clinical indications for adjunctive use of BoNT in pediatric patients.
Precise delivery of BoNT into targeted muscles provides a marked local improvement in spasticity while reducing the probability of undesired effects in adjacent muscles and adverse systemic side effects.
Advertisement

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/17f8b1d8-1ee4-4085-83f1-c86545430c76/15-NEU-2527-Aldosari-Inset1_jpg)
Figure 1. Injection of the gastrocnemius muscle using ultrasound guidance.
Correct needle placement (Figure 1), especially in small or deep-seated muscles, is challenging, even for an experienced operator. Several studies have shown that use of anatomical landmarks and muscle palpation alone provides inadequate guidance for reliable needle placement. In 2005, Chin and colleagues found that needle placement by anatomic localization alone failed in 22 percent of cases when the gastroc-soleus was injected, and it failed in at least 87 percent of cases when the tibialis posterior muscle or the flexor carpi radialis muscle was injected.
Electromyography and electrical muscle stimulation provide effective guidance and are widely used in the adult population. These methods have limited use in children, however, because they are painful and time-consuming and require the patient’s cooperation. Of the other imaging techniques explored as potential alternatives in pediatric cases, particularly to guide injections into deep-seated muscles, ultrasound has proved to be the most convenient and practical.
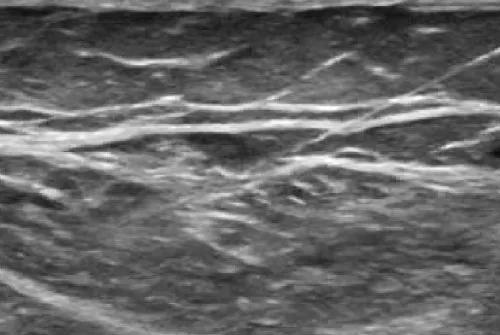
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/da0ced98-1ca9-4fc0-9bda-9e422a43bf15/15-NEU-2527-Aldosari-Inset2_jpg)
Figure 2. Ultrasound imaging during gastrocnemius muscle injection, allowing precise needle placement (needle is shown entering from the upper right corner).
Ultrasound provides information about muscle size and fibrosis, both of which can be important factors in decision-making. The modality also enables the operator to directly visualize the entire process, including needle placement. This allows the operator to gain a better understanding of the individual’s anatomy while performing the injection, facilitating target selection and further improving injection technique (Figure 2).
Advertisement
In patients who are uncooperative or sedated, ultrasound can be very helpful in identifying small muscles involved in spasticity and focal dystonia, such as single fascicles of finger flexors. Ultrasound also allows clear differentiation of structures near target muscles, making it helpful in preventing subcutaneous or intravenous injection.
Ultrasound guidance can likewise help avoid the pain that arises when the needle comes into contact with the periosteum, and in cases where the psoas muscle is injected, ultrasound imaging safeguards against accidental injection into the intestines.
Dr. Aldosari is a staff pediatric neurologist and pediatric movement disorders specialist with Cleveland Clinic’s Pediatric Neurosciences Program.
Koman LA, Mooney JF 3rd, Smith B, et al. Management of cerebral palsy with botulinum-A toxin: preliminary investigation. J Pediatr Orthop. 1993;13:489-495.
Elovic EP, Esquenazi A, Alter KE, et al. Chemodenervation and nerve blocks in the diagnosis and management of spasticity and muscle overactivity. PM R. 2009;1:842-851.
Copeland l, Edwards P, Thorley M, et al. Botulinum toxin A for nonambulatory children with cerebral palsy: a double blind randomized controlled trial. J Pediatr. 2014;165:140-146.
Berweck S, Feldkamp A, Francke A, et al. Sonography-guided injection of botulinum toxin A in children with cerebral palsy. Neuropediatrics. 2002;33:221-223.
Santamato A, Micello MF, Panza F, et al. Can botulinum toxin type A injection technique influence the clinical outcome of patients with post-stroke upper limb spasticity? J Neurol Sci. 2014;347:39-43.
Advertisement
Chin TY, Nattrass GR, Selber P, Graham HK. Accuracy of intramuscular injection of botulinum toxin A in juvenile cerebral palsy: a comparison between manual needle placement and placement guided by electrical stimulation. J Pediatr Orthop. 2005;25:286-291.
Advertisement
Advertisement

New study advances understanding of patient-defined goals

Testing options and therapies are expanding for this poorly understood sleep disorder

Real-world claims data and tissue culture studies set the stage for randomized clinical testing

Digital subtraction angiography remains central to assessment of ‘benign’ PMSAH

Cleveland Clinic neuromuscular specialist shares insights on AI in his field and beyond

Findings challenge dogma that microglia are exclusively destructive regardless of location in brain

Neurology is especially well positioned for opportunities to enhance clinical care and medical training

New review distills insights from studies over the past decade