Locations:

Serum calcium monitoring important in hypoparathyroidism

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/28da0419-ffcb-4013-b33b-50186d3f5ebe/hypercalcemia_650x450_jpg)
hypercalcemia_650x450
By Laurence (Ned) Kennedy, MD, and Karla Arce, MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
A 28-year-old woman who had recently given birth was referred to our Endocrine Calcium Clinic for newly noted hypercalcemia. She had been diagnosed with DiGeorge syndrome when she was 6 weeks old, after presenting with seizures. Hypoparathyroidism was confirmed at that time, and she had been treated with calcium and calcitriol at various doses over the years.
During the pregnancy, her medication dosages had required frequent adjustments. Prior to evaluation at our clinic, she was taking 0.25 mcg of calcitriol daily, 12.5 mg of hydrochlorothiazide (HCTZ) daily, 250 mg of magnesium three times a day (TID) and 750 mg of calcium carbonate TID.
The pregnancy was uncomplicated. She delivered a baby girl at term and began breast-feeding immediately. At that time, her serum calcium was 8.6 mg/dL (8.5-10.1 mg/dL), phosphorus was 3.4 mg/dL (2.5-2.9 mg/dL) and magnesium was 1.6 mg/dL (1.7-2.4 mg/dL). Two weeks postpartum, the patient’s serum calcium had increased to 12.7 mg/dL, at which time she was referred to our clinic.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/3959b01b-c9e8-4800-9d65-655340343602/calcium_chart_805x600_jpg)
We decreased the calcitriol to 0.25 mcg every other day. Six weeks later, she remained hypercalcemic (13.1 mg/dL), so calcium carbonate was stopped and the 0.25 mcg of calcitriol was decreased to every three days. She continued to breastfeed for 12 months and her calcitriol requirements gradually increased, reaching pre-pregnancy levels within days of weaning at 13 months post-partum.
DiGeorge syndrome is a rare condition caused by an embryologic defect in the development of the third, fourth and fifth branchial pouches. One of its major manifestations is hypoparathyroidism.
Advertisement
Maternal hypoparathyroidism may change during pregnancy due to increased intestinal absorption of calcium; this may be mediated by 5-dihydroxyvitamin D due to parathyroid hormone-related peptide (PTHrP) secretion from the placenta and the myometrium. High concentrations of PTHrP have been found in human breast milk, and this may be the principal factor involved in the transfer of calcium from the mammary glands to milk. There is evidence that PTHrP secretion depends strongly on the action of prolactin.
This case illustrates the importance of monitoring serum calcium closely in patients with hypoparathyroidism during pregnancy and, particularly, lactation. Calcitriol requirements of hypoparathyroid women fall early in the postpartum period, especially if the woman breast-feeds, and hypercalcemia may occur if the calcitriol dosage is not reduced.
Dr. Arce is a former fellow in the Department of Endocrinology, Diabetes and Metabolism at Cleveland Clinic.
Advertisement
Advertisement

Radiofrequency ablation significantly reduces symptom severity, shrinks nodules

Maternal-fetal medicine specialists, endocrinologists and educators team up

Giving young patients a hand as they take charge of their own health

Case illustrates how easily condition can mimic preeclampsia
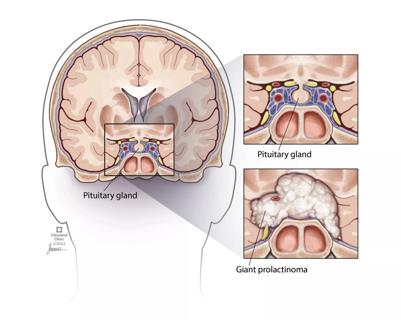
Analysis examines surgical resection of rare pituitary tumors
Screening and medication key to better outcomes

Spinal cord stimulation can help those who are optimized for success
Incidence, outcomes and management