Locations:

Differential diagnosis should include vascular diseases
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/e92bab78-3ae1-4df0-aaa7-0f513f852569/Vascular-690x380_jpg)
Vascular-690×380
Fibromuscular dysplasia (FMD) should be on every primary care physician’s radar because it can lead to spontaneous coronary artery dissection (SCAD). More than 90 percent of FMD patients are women.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“FMD is terribly under-recognized and underdiagnosed,” says vascular medicine specialist Heather L. Gornik, MD, Medical Director of the Noninvasive Vascular Laboratory in Cleveland Clinic’s Sydell and Arnold Miller Family Heart & Vascular Institute. “The U.S. Fibromuscular Dysplasia Registry shows about a four-year lag between the time patients present with symptoms and diagnosis.”
FMD, a nonatherosclerotic arterial disease affecting medium-size vessels, most often involves the renal, carotid and vertebral arteries. FMD may progress to arterial stenosis, beading, aneurysm and, in some cases, dissection.
“Unfortunately, FMD is not high on the differential diagnosis. The presenting symptoms can be easily attributed to other diseases,” says Dr. Gornik.
In addition, symptoms are often addressed individually rather than in the context of a larger clinical picture. The symptoms of FMD include:
The one differentiating symptom of FMD is pulsatile tinnitus, which affects over one third of FMD patients. Pulsatile tinnitus is rare in the general population. However, Dr. Gornik notes that 5.6 percent of patients with FMD are completely asymptomatic.
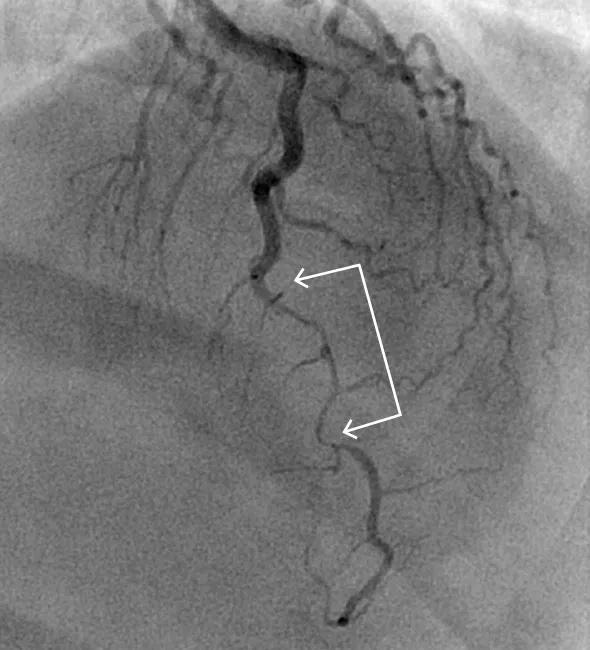
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/472b738f-3125-41ef-873d-96bf1f1697e6/inset2_jpg)
Coronary angiogram of 35-year-old woman who presented with acute coronary syndrome. There is a type 2 coronary dissection in the mid and distal left anterior descending artery.
SCAD occurs when a tear develops in the innermost layer of a coronary arterial wall or when there is internal bleeding between the wall’s layers, disrupting or blocking blood flow to the heart.
As in FMD, the vast majority of patients who develop SCAD are women. The average age of women who are affected is around 50.
Advertisement
“SCAD is a challenging diagnosis for a number of reasons. While its appearance is very obvious on some coronary angiograms, on others it can mimic plaque or mild coronary artery disease caused by atherosclerosis,” says women’s cardiovascular medicine specialist Esther (Soo Hyun) Kim, MD, MPH, of the Heart & Vascular Institute’s Section of Vascular Medicine and Section of Preventive Cardiology.
She notes that SCAD generally manifests as a heart attack, so when any young woman presents with a heart attack but has few to no traditional risk factors for atherosclerosis, physicians should include SCAD in the differential diagnosis.
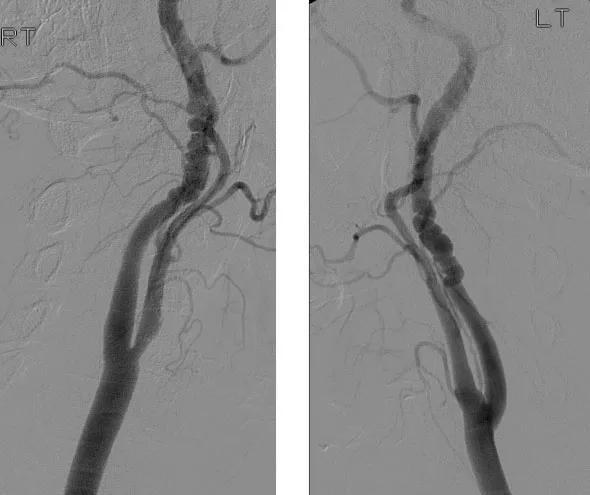
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/6208a54b-e53a-48af-9ebb-832f0d82ff5e/inset1_jpg)
Angiograms showing bilateral multifocal FMD of the internal carotid arteries (“string of beads”).
Stents are effective in opening coronary obstruction from atherosclerotic plaque, but they can worsen the dissection in SCAD, triggering more severe obstructions. For this reason, stenting is reserved for severe cases, when SCAD causes persistent pain or when signs indicate the patient is not doing well.
Experts do not yet understand all the underlying causes of SCAD. However, in some cases, SCAD can occur because of arterial weakening due to:
SCAD also has been associated with extreme physical or emotional stress.
“While not all SCAD is from FMD, I think we are learning that SCAD is probably a variant presentation of FMD. Some data suggest that if you look at all the arteries
in SCAD patients, 70 percent of the time you will find FMD,” says Dr. Kim.
Advertisement
“However, if you take FMD patients and ask if they have had SCAD, far fewer will cite a history of SCAD. There is clearly a disconnect.”
Drs. Gornik and Kim stress the importance of prompt referral for patients with FMD and SCAD.
Medical treatment is usually effective in SCAD. Dr. Kim is enrolling patients in a comprehensive SCAD study that is following patients long-term to gain a better understanding of the natural history.
FMD and SCAD require multidisciplinary management. Since 2008, Cleveland Clinic’s FMD Clinic has offered patients with FMD access to a team of vascular medicine specialists, vascular surgeons, nephrologists, neurologists and neurosurgeons, interventional cardiologists, medical geneticists and other specialists.
To refer patients with FMD or SCAD to Cleveland Clinic, please call 855.REFER.123.
Advertisement
Advertisement

A sampling of outcome and volume data from our Heart & Vascular Institute

Concomitant AF ablation and LAA occlusion strongly endorsed during elective heart surgery

Large retrospective study supports its addition to BAV repair toolbox at expert centers

Young age, solid tumor, high uptake on PET and KRAS mutation signal risk, suggest need for lobectomy

Surprise findings argue for caution about testosterone use in men at risk for fracture

Residual AR related to severe preoperative AR increases risk of progression, need for reoperation

Findings support emphasis on markers of frailty related to, but not dependent on, age

Provides option for patients previously deemed anatomically unsuitable