Locations:

Growing experience supports procedure’s safety and efficacy
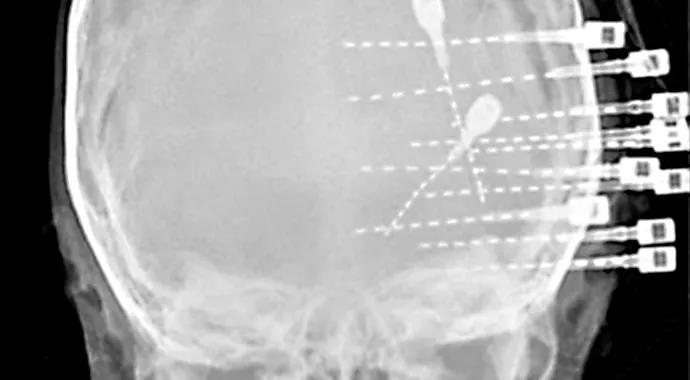
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/4d251aab-c575-41f9-bc5e-fe61dd1cbe10/Lachhwani-690x380_jpg)
Lachhwani-690×380
By Deepak Lachhwani, MD, and Jorgé Gonzalez-Martinez, MD, PhD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Stereoelectroencephalography (SEEG) is a methodology for exploring surgical resection strategy in medically refractory patients suspected to have focal epilepsy. SEEG involves the temporary surgical implantation of electrodes that enable simultaneous recording of electrical activity from many parts of the brain at high temporal resolution (~1 ms), which is used to identify the epileptogenic zone.
SEEG involves relatively minimal risk of morbidity and mortality, and its results have aided the planning of surgical resection in appropriate candidates and the decision to avoid resection in patients deemed to have a poor prognosis.
Our institution has seen a steady growth and acceptance of this methodology based on some distinct merits of SEEG compared with other methods of invasive evaluation, such as subdural grids.
In our recently published series of 28 pediatric patients who underwent SEEG evaluation, 18 of 28 were able to undergo resection, 13 of 18 had improvement in their seizure control and 5 of 18 were seizure-free.
Careful review of patient profiles highlighted that SEEG-related advantages are especially relevant in young patients such as BB, who is featured in Figures 1 and 2. By the age of 2 years 5 months, BB had failed multiple seizure medications and the first attempt at tailored resection (guided by subdural grids) of the presumed seizure focus in her left frontal lobe. Frequent and intense daily seizures caused a significant impairment in her quality of life.
BB’s family arrived at our institution for a second opinion, and we recommended SEEG as the methodology of choice to explore surgical treatment options. At the age of 3 years 4 months, BB became the youngest of our patients to undergo successful SEEG implantation, followed by resection within six weeks. Since surgery, she has remained seizure-free for more than 18 months.
Advertisement

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/56fc5391-42d1-49e4-ab3a-9ec00bbea686/Lachhwani-fig1_jpg)
Figure 1. Image of patient BB at 3 years 4 months of age. Photo in an operating room showing the implanted SEEG electrodes.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/830a4286-b40c-4543-bbc4-be8ed5e14bbd/Lachhwani-fig2_jpg)
Figure 2. Skull X-ray demonstrating positioning of the SEEG electrodes. BB has remained seizure-free for more than 18 months since her surgery.
Our experience with SEEG has provided these insights:
Advertisement
In conclusion, our ongoing experience weighs strongly in favor of SEEG as a safe and effective methodology for identifying young candidates suitable for surgical treatment of refractory epilepsy.
Dr. Lachhwani is a pediatric epileptologist and Chief of Neurology at Cleveland Clinic Abu Dhabi.
Advertisement
Advertisement

New study advances understanding of patient-defined goals

Testing options and therapies are expanding for this poorly understood sleep disorder

Real-world claims data and tissue culture studies set the stage for randomized clinical testing

Digital subtraction angiography remains central to assessment of ‘benign’ PMSAH

Cleveland Clinic neuromuscular specialist shares insights on AI in his field and beyond

Findings challenge dogma that microglia are exclusively destructive regardless of location in brain

Neurology is especially well positioned for opportunities to enhance clinical care and medical training

New review distills insights from studies over the past decade