Locations:

Three case presentations demonstrate techniques
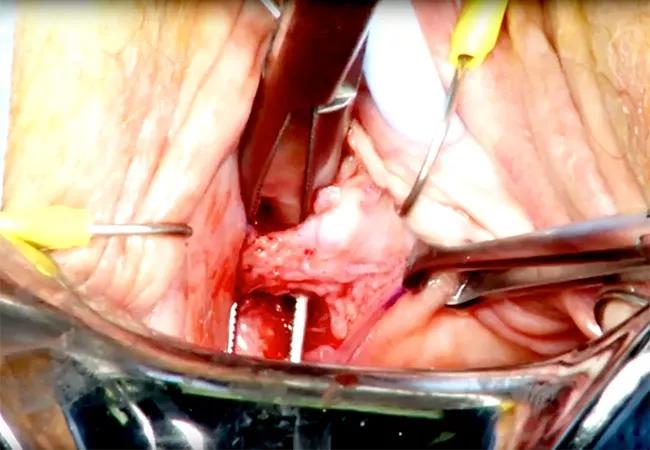
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/d34e88a3-8861-49f5-9a83-b5978e387092/650x450-Sling-Excision_jpg)
650×450-Sling Excision
Synthetic midurethral sling placement is the most common procedure performed for women with symptomatic stress urinary incontinence.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Postoperative complications are well-documented in the literature. The estimated rate of sling removal for urethral obstruction is approximately 2.3 percent, and for mesh extrusion is 1.8 percent. However, this may be an underestimate of the true incidence of these complications.
Surgeons at Cleveland Clinic’s Glickman Urological & Kidney Institute perform transvaginal sling excision on patients with evidence of sling obstruction or mesh extrusion.
This video presents three separate cases of synthetic mesh excision and provides tips to improve surgical outcomes in patients. This video was presented at the American Urological Association’s 2016 annual meeting and received an award for best video within its section.
Video content: This video is available to watch online.
View video online (https://www.youtube.com/embed/uky9uDsy9PI?feature=oembed)
The first patient underwent transobturator sling surgery in 2010 for symptomatic stress incontinence. Postoperatively, she developed voiding dysfunction. Once her catheter was removed, she passed the voiding trial. She was evaluated for urinary hesitancy and weak stream. Her postoperative force of stream was 40 percent of the original.
She presented with urinary hesitancy and weak stream. Her office cystoscopy was negative for mesh perforation, and her urodynamics study showed evidence of outlet obstruction. She elected to proceed with excision of a portion of the sling. Watch the video for detailed, step-by-step surgical instruction of how they treated this patient.
The second case was of a patient who underwent transobturator sling surgery for mixed urinary incontinence and had significant worsening of urgency incontinence postoperatively. The third case discussed was of a patient who underwent sling placement for stress incontinence but whose husband complained of feeling the mesh during sexual intercourse. Watch the video to learn how surgeons handled both cases.
Advertisement
Advertisement

Clinicians should individualize dosing practices based on patient risk factors and preferences
Pioneering and refining the approach in pyeloplasty, nephrectomy and more
Fully-automated process uses preop CT, baseline GFR to estimate post-nephrectomy renal function

Could mean earlier treatment, but also could have negative effects

Unlike earlier pills, new drugs do not cause liver toxicity

Male factors play a role in about half of all infertility cases, yet men often are not evaluated
Surgeons choreograph nearly simultaneous procedures, sharing one robot between two patients

Identifying barriers in the renal genetic assessment of Black patients