Locations:

A complex case muddied by myriad comorbidities
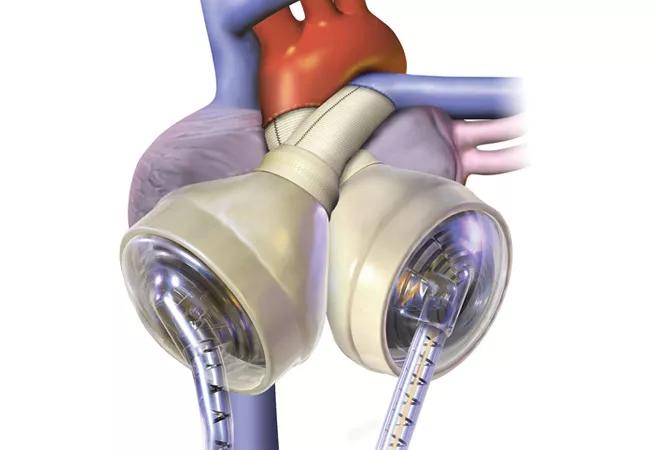
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/6dd061db-5248-49f6-b0a6-8449f7d8adf2/16-HRT-2449-TAH-CQD-650p_jpg)
Total Artificial Heart as Bridge to Transplant in Biventricular Heart Failure
By Nader Moazami, MD; Edward Soltesz, MD; and Miriam Jacob, MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
A 57-year-old man diagnosed in 2008 with viral cardiomyopathy subsequently developed progressive nonischemic cardiomyopathy. In early 2015, he reported symptoms consistent with atrial fibrillation and underwent ablation and implantable cardioverter-defibrillator (ICD) placement. In mid-April 2015, he was admitted to his local hospital with cardiogenic shock and treated with dobutamine and diuretics. Nevertheless, his condition continued to deteriorate rapidly. He developed biventricular heart failure and was placed on extracorporeal membrane oxygenation (ECMO) support and was transferred to Cleveland Clinic in late April for further management.
On arrival, the patient was cachectic and in renal and liver failure. Although he was intubated, his neurological function was intact, and he was able to understand and consent to a plan of care. One week after his arrival, ECMO and his ICD were removed and his heart was replaced with a SynCardia temporary Total Artificial Heart (TAH) (image at top of post) as a bridge to transplantation.
Over the succeeding weeks, the patient had a complicated recovery that included respiratory failure, pneumonia, leukocytosis and dysphagia. With aggressive resuscitation and multidisciplinary management, he continued to overcome these complications, and his liver and renal function improved with the TAH therapy. With aggressive additional in-hospital physical therapy, he improved to the point that in late July he was listed as UNOS status 1A for heart transplantation.
Advertisement
In mid-August, the TAH driver was changed to SynCardia’s portable Freedom® driver, with the goal of allowing the patient to wait for a donor heart at home. Ultimately, he and his wife felt insecure about leaving the hospital and decided to wait at Cleveland Clinic.
In early October, five months after his admission to Cleveland Clinic, the patient’s TAH was explanted and replaced with a healthy, well-functioning donor heart. Although this was a complex reoperation, he quickly improved after transplantation and was discharged home in mid-November 2015 on typical post-transplant medications with prescriptions for home occupational, physical and speech therapy.
One year later, the patient returned for a checkup. He was back to normal activity, eating well, symptom-free and in good spirits.
This patient presented multiple challenges. He was initially too sick to transplant, with severe biventricular failure. A TAH was his only salvage option. These devices have proved highly effective as rescue therapy in patients with biventricular failure. However, because patients like this typically spend months in the hospital to recuperate, success with a TAH requires cooperative, resilient and motivated patients (and families) who are able and willing to work hard to improve and strengthen themselves in preparation for transplant.
Heart transplantation following removal of a TAH is challenging, in view of the significant inflammatory response to the device and the extensive fibrosis that obliterates all surgical planes.
Advertisement
Although this patient’s case appears dramatic, it is typical of the complex patients we see every day and illustrates the dual strengths of Cleveland Clinic’s Cardiac Transplantation and VAD Program:
These qualities enable us to tailor therapy for very sick patients with varying physiologies and indications.
Our heart transplant team comprises three surgeons and 12 cardiologists. The cardiologists rotate weekly, which allows them to become familiar with every patient. They are supported by a superb staff of mechanical support nurse practitioners who manage day-to-day care. The transplant team meets daily to discuss how best to achieve our common goal of stabilizing patients, transplanting them and sending them home.
This patient’s array of serious comorbidities underscores the importance of supportive staff and multidisciplinary specialty expertise for advanced heart failure care. Our cardiac anesthesiologists are comfortable with the challenges of anesthetizing patients on mechanical support devices and those undergoing heart transplant. Their expertise in the surgical ICU is invaluable. We likewise count on expert colleagues from Cleveland Clinic’s infectious disease, nephrology, gastroenterology, pulmonary medicine and other specialty programs to help resolve the multiple medical issues that so often accompany advanced heart failure.
By working together, we aim to ensure that these extremely fragile patients receive optimal care around the clock during extended hospitalization and after discharge.
Advertisement
Dr. Soltesz is a cardiothoracic and heart transplant surgeon in Cleveland Clinic’s Department of Cardiothoracic Surgery. Dr. Jacob is a cardiologist in the Section of Heart Failure and Transplant Medicine.
Image courtesy of syncardia.com.
Advertisement
Advertisement

A sampling of outcome and volume data from our Heart & Vascular Institute

Concomitant AF ablation and LAA occlusion strongly endorsed during elective heart surgery

Large retrospective study supports its addition to BAV repair toolbox at expert centers

Young age, solid tumor, high uptake on PET and KRAS mutation signal risk, suggest need for lobectomy

Surprise findings argue for caution about testosterone use in men at risk for fracture

Residual AR related to severe preoperative AR increases risk of progression, need for reoperation

Findings support emphasis on markers of frailty related to, but not dependent on, age

Provides option for patients previously deemed anatomically unsuitable