Locations:

A closer look at valve repair and replacement for ToF
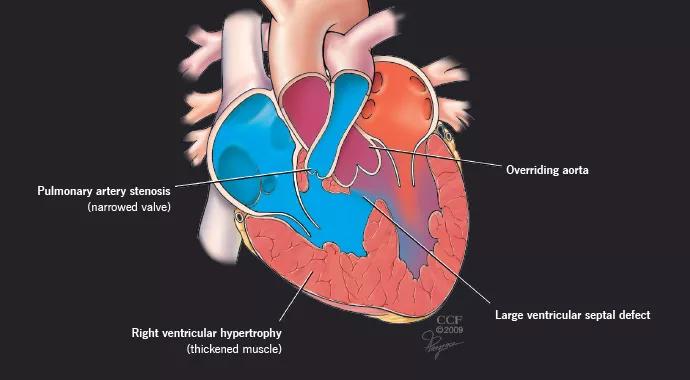
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/2ef9f647-851d-4589-80ae-17fe6988b6a7/ToF-690x380_jpg)
ToF-690×380
By Gösta Pettersson, MD, PhD, and Richard Krasuski, MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Tetralogy of Fallot (ToF) is the most common complex lesion seen in adults with congenital heart disease (CHD). The condition usually is diagnosed at birth or shortly thereafter in response to its hallmark cyanosis.
It is sometimes treated with a shunt, and palliative surgery typically is performed between 3 and 9 months of age. These techniques can relieve symptoms for years of 10 well into adulthood, until more definitive surgical repair is needed. If necessary, a valve repair (or replacement) to open the outflow tract can be performed starting from approximately age 5 or 6 years.
In keeping with the above, the large majority of adults with ToF evaluated at Cleveland Clinic’s Adult Congenital Heart Disease Center have undergone palliative or corrective surgery for the condition during childhood. Yet the occasional patient with ToF reaches adulthood without prior diagnosis or surgical repair; these patients may or may not be symptomatic when referred.
During the past several years, we have seen a handful of adults with ToF who were not previously diagnosed — or fully diagnosed — and thus had not undergone surgical correction.
While it is highly unusual for ToF to go undiagnosed until adulthood, it does happen — typically in cases such as this when there is a perfect balance in childhood between the narrowing of the pulmonic valve and the ventricular septal defect so that cyanosis does not occur.
One patient was fortunate to have avoided the complications that can be associated with uncorrected ToF, which include atrial clot formation, increased risk of infections and abscesses, or even sudden death.
Advertisement
Much more commonly, the adults we see with ToF were diagnosed early in life due to cyanosis, and they have received palliative — and most often also corrective —surgery. We see these patients for routine follow-up and for long-term complications that can arise from either the disease or prior surgeries.
When ToF is repaired in childhood, we try to spare the pulmonic valve, but more often the pulmonic valve is opened up and an outflow patch is placed, which compromises the valve’s function. (Valve placement in childhood is rare because it is not necessary in the short term and the available valves have very limited life spans.) Therefore, leaky valves are the most common reason these patients are referred for surgical repair in adulthood.
We determine and continually monitor the need for a valve repair or replacement based primarily on symptoms such as cyanosis or fatigue, physical ability and size of the right ventricle. Some patients may never need a reoperation.
However, it is important that surgical intervention, if needed, occur before the right ventricle becomes too stretched.
We always strive for valve-sparing surgeries; in cases when the pulmonary arteries and right ventricle are in good condition, patients can go through life without ever requiring a prosthetic valve. Occasionally we are able to implant a valve without performing surgery, but the ability to replace the valve percutaneously is often limited by the large size of the pulmonary outflow tracts or by other structural defects that need to be concomitantly corrected.
Advertisement
In certain cases in which we know additional strain may be placed on the heart in the near future — such as a planned pregnancy — we may recommend valve replacement surgery sooner than we otherwise would.
Regardless of when ToF is diagnosed, patients who require interventional or surgical procedures are best served at centers with a specialized multidisciplinary adult CHD center, as recommended by the American College of Cardiology/American Heart Association guidelines on adult CHD. Because this specialty is fairly uncommon, at least 30 percent of the patients seen at our center come from out of state.
When performed by an experienced CHD surgeon, surgical repair of ToF in adults has a high success rate, and most patients will not need further surgical treatment.
Advertisement
Advertisement

A sampling of outcome and volume data from our Heart & Vascular Institute

Concomitant AF ablation and LAA occlusion strongly endorsed during elective heart surgery

Large retrospective study supports its addition to BAV repair toolbox at expert centers

Young age, solid tumor, high uptake on PET and KRAS mutation signal risk, suggest need for lobectomy

Surprise findings argue for caution about testosterone use in men at risk for fracture

Residual AR related to severe preoperative AR increases risk of progression, need for reoperation

Findings support emphasis on markers of frailty related to, but not dependent on, age

Provides option for patients previously deemed anatomically unsuitable