Locations:

Findings suggest that the effectiveness of interventions may depend more on the frequency and delivery methods of the intervention rather than who is delivering the intervention

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/d7d6c862-16bc-40d4-9634-b74d1783159d/21-EMI-2376855-CQD-Hero-650x450-1_jpg)
Diabetes care
The importance of collaboration with non-physician providers in caring for patients with type 2 diabetes mellitus (T2DM) has been demonstrated again in a recently published systematic review meta-analysis. The review, which investigated the effect of interventions to overcome therapeutic inertia on glycemic control in individuals with T2DM, was published in Diabetes, Obesity and Metabolism.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Diabetes continues to be one of most prevalent health issues, despite much effort to reduce the adverse outcomes associated with T2DM – micro- and macro-vascular complications, excess mortality, and increased costs of care to the healthcare system. Therapeutic inertia, the failure of healthcare providers to initiate or intensify treatment when indicated or to deescalate therapy when appropriate, greatly contributes to the disparity between population health goals for diabetes and its current status. The problem is multifactorial and stems from patient-level factors, provider-level factors and system-level factors.
The systematic review and meta-analysis focused on peer-reviewed journal publications between January 1, 2004 and December 31, 2019. Studies were selected that evaluated the effect of interventions on glycated hemoglobin (HbA1c) control and that tested the effect of interventions in healthcare settings and included providers (primary care physicians, endocrinologists, nurse practitioners, physician assistants, clinical pharmacists, diabetes educators and nurses) commonly involved in the therapeutic management of diabetes.
Thirty six studies were included in the analysis. From those studies, 22,243 individuals were combined in non-linear random-effects meta-regressions. The median duration of intervention was one year (0.9 months to 36 months). Compared to the control arm, HbA1c reduction was observed with nurse- or CDE-based interventions, care management and patient education interventions, pharmacist-based interventions and physician-based interventions. Across the included studies, a reduction in HbA1c was observed only during the first year and in individuals with pre-intervention.
Advertisement
Compared to the control arm, HbA1c reduction ranged from: -1.62% to -0.40% for nurse- or CDE-based interventions; -1.20% to 0.30% for care management and patient education interventions; -0.90% to -0.60% for pharmacist-based interventions; -0.40% to 0.26% for physician-based interventions. Across the included studies, a reduction in HbA1c was observed only during the first year (6 months: -0.38%, 95% CI -0.56, -0.20; 1 year: -0.15%, 95% CI -0.30, 0.01 and in individuals with pre-intervention HbA1c >9%.
“Regardless of the type of intervention, we found the reduction of HbA1c was greatest during the first year and in individuals with pre-intervention HbA1c >9%,” says Kevin M. Pantlone, DO, FACE, a staff endocrinologist and Director of Diabetes Initiatives in Cleveland Clinic’s Endocrinology & Metabolism Institute, and one of the authors of the study. Dr. Pantalone also serves as vice-chair of the Overcoming Therapeutic Inertia Steering Committee for American Diabetes Association. “We believe this is likely because the degree of modifiable risk may influence how successful the strategy is. Additionally, it may be that these patients with higher HbA1c or patients whose intervention strategies occur earlier in their treatment have the most room for improvement. ”
Dr. Pantalone also suggests that the effectiveness of interventions may not only depend on the intervention, or delivery methods and frequency of the intervention, but rather who is delivering the intervention.
“We found that the most effective approaches to reducing therapeutic inertia and improving HbA1c were interventions where non-physicians such as nurses, pharmacists or certified diabetes educators (CDEs) had autonomy to independently begin or intensify treatment,” says Dr. Pantalone. “In one of our included studies, it was determined that simply including non-physician team members in diabetes care teams is not sufficient to improve diabetes outcomes. Rather, those team members must also be empowered to implement guideline-based medication changes.” Moreover, while not all of the included studies reported frequency of patient communication between the arms of the study, among those that did effectively, interventions often included in-person or phone communication with a care team member on a regular basis.
Advertisement
Improving education – both in terms of patient and provider – also was associated with a reduction of HbA1c. However, Dr. Pantalone notes that there are varying levels of success associated with different methods of changing clinician behavior. “Education, feedback or quality improvement activities were actually least likely to be associated with improvements in HbA1c compared to usual care,” says Dr. Pantalone. “We found that variation in the effectiveness of physician-based interventions may be driven in large part by the intensity of the intervention. For example, the most effective clinician education intervention involved one-on-one guidance provided by endocrinologists to internal medicine residents practicing in a primary care practice. This suggests that education tools can be effective, but they likely require significant investments in both time and personnel. This dilemma is why it is important to empower pharmacists, nurses, diabetes educators, advanced practicing providers and other members of the diabetes care team, with the ability to initiate and intensify treatment, supported by appropriate guidelines, protocols and collaborative agreements. ”
Advertisement
Advertisement

Radiofrequency ablation significantly reduces symptom severity, shrinks nodules

Maternal-fetal medicine specialists, endocrinologists and educators team up

Giving young patients a hand as they take charge of their own health

Case illustrates how easily condition can mimic preeclampsia
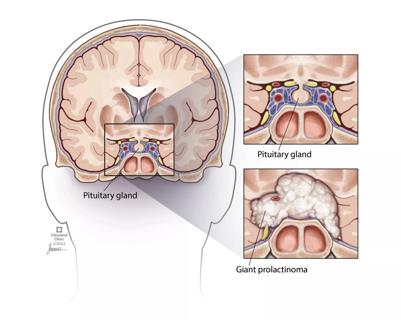
Analysis examines surgical resection of rare pituitary tumors
Screening and medication key to better outcomes

Spinal cord stimulation can help those who are optimized for success
Incidence, outcomes and management