Locations:

ENRICH trial of an MIS approach aims to find out
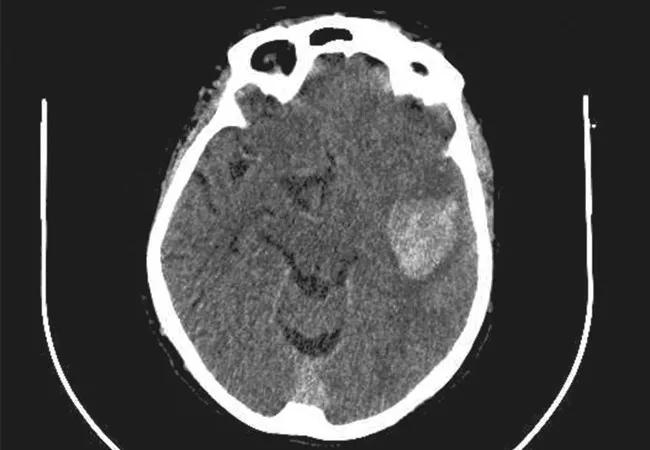
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/34f311e9-3861-4795-a1a1-8f312afbbff9/17-NEU-902-Bain-650x450_jpg)
17-NEU-902-Bain-650×450
Can early surgical hematoma evacuation in intracerebral hemorrhage (ICH) be done in such a minimally invasive fashion that it promises significantly more benefit than risk?
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
That’s what Cleveland Clinic and nine other major U.S. medical centers hope to find out by participating in the Early Minimally Invasive Removal of Intracerebral Hemorrhage (ENRICH) study, a phase 3 clinical trial comparing a novel surgical system for clot removal within 24 hours of a hemorrhagic stroke to standard medical management. The system involves specialized devices designed to be manipulated through a small opening in the skull for gentle evacuation of the hematoma with minimal tissue damage.
“Historically, surgery was not a viable option for intracerebral hemorrhage because of damage caused by the surgery itself,” says Mark Bain, MD, a staff neurosurgeon in Cleveland Clinic’s Cerebrovascular Center who’s serving as the site’s principal investigator for the trial. “The system tested in ENRICH offers a minimally disruptive approach to the hematoma, fine control, and a gentle way to remove the hemorrhage. We have high hopes it will prove to be a better treatment for these devastating strokes.”
ICH is the most lethal form of stroke, resulting in death in one-third to one-half of victims and grave disability in many survivors. Following a sudden bleed in the brain, primary injury occurs within minutes to hours because of mechanical damage, oxygen loss, swelling and tissue death. Over the ensuing days, the trapped blood clot causes a host of secondary problems by releasing multiple factors that lead to inflammation and further tissue destruction.
Although it’s long been thought that surgical hematoma removal at the time of stroke could prevent damage, technical problems have proved daunting. Previous surgical trials have often demonstrated no benefit from surgical intervention when compared with a “wait and see” medical strategy, Dr. Bain explains.
Advertisement
The ENRICH trial is comparing parafascicular, transsulcal surgery using NICO Corporation’s BrainPath® access technology (detailed below) to standard medical management for ICH (based on the Clinical Standardization Guidelines as adapted by Emory University from the 2015 AHA/ASA Guidelines for the Management of Spontaneous Intracerebral Hemorrhage).
The experimental surgery, to be administered within 24 hours after onset of stroke symptoms, consists of the following steps:
“The system is very well thought out,” notes Dr. Bain, who received two days of specialized, hands-on training in the use of the BrainPath technology. All surgeons in the study undergo similar training, with experience on at least 10 patients required before they may participate in the trial.
Advertisement
The study will enroll 300 adult patients and is anticipated to run for two to three years. Release of an interim analysis is expected after the first 100 to 150 patients. The adaptive study design will allow for inclusion and exclusion criteria to change during the trial, depending on results.
Clinical efficacy will be determined by demonstrating a 10 percent improvement in functional outcome as measured by blinded assessment six months after stroke onset using the modified Rankin Scale.
Secondary outcome measures include mortality rate at 30 days, change of hemorrhage volume between the index CT and 24-hour follow-up CT, and cost per quality-adjusted life-year gained.
Two previous small trials evaluating the BrainPath approach for ICH demonstrated very low mortality rates and functional benefits. In an uncontrolled multicenter pilot study of 39 patients (Neurosurgery. 2017;80:515-524), more than half had good functional recovery and no deaths occurred, despite patient characteristics that predicted a 26 percent mortality rate with standard care. A separate series of 18 patients at Cleveland Clinic (Oper Neurosurg [Hagerstown]. 2017;13:69-76) demonstrated similar successful outcomes and one death.
Dr. Bain expects the ENRICH trial will strengthen the favorable findings from these early studies and lead to a new standard of care for early ICH treatment.
“Results of this trial could revolutionize the world of hemorrhagic stroke treatment,” he says.
Advertisement
Advertisement

New study advances understanding of patient-defined goals

Testing options and therapies are expanding for this poorly understood sleep disorder

Real-world claims data and tissue culture studies set the stage for randomized clinical testing

Digital subtraction angiography remains central to assessment of ‘benign’ PMSAH

Cleveland Clinic neuromuscular specialist shares insights on AI in his field and beyond

Findings challenge dogma that microglia are exclusively destructive regardless of location in brain

Neurology is especially well positioned for opportunities to enhance clinical care and medical training

New review distills insights from studies over the past decade