Locations:

A novel approach to EVAR aims to reduce risks
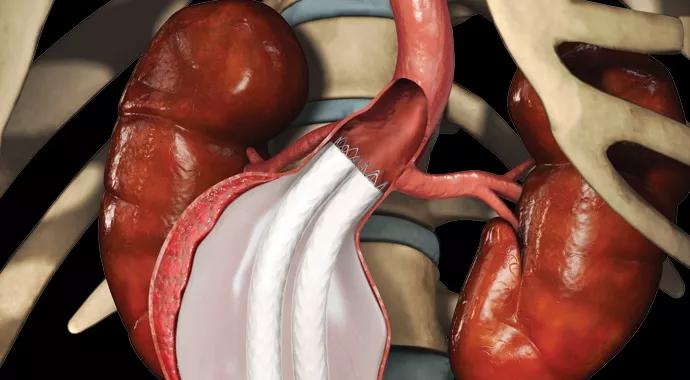
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/cf645c5a-b0fe-487f-aeca-c1a089f8401f/endoleaks-690x380_jpg)
endoleaks-690×380
A new approach to endovascular aneurysm repair (EVAR) could significantly reduce the risk of endoleaks and stent graft migration.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
EVAR has revolutionized abdominal aortic aneurysm (AAA) treatment. The technique delivers a fabric-covered stent to the aneurysm site via a catheter, after which the stent is expanded inside the aneurysm sac to provide a new conduit for blood flow. The stent graft seals the aortic blood flow from entering the aneurysm, but it cannot prevent blood flow from small branches that perfuse the aneurysm.
In typical endograft treatment of AAA, about 15 to 20 percent of patients develop this type of flow into the aneurysm sac, referred to as a type II endoleak. It is not strictly a leak, as the flow is still in the vascular system, but it is in the aneurysm, outside the endograft.
“These ‘leaks’ can lead to pressurization of the aneurysm sac and, in some instances, to continued increase in the aneurysm’s size,” explains Daniel Clair, MD, Chair of Vascular Surgery at Cleveland Clinic. “In fact, in studies of patients with these types of leaks, the risk of complications and mid- to long-term graft failure is increased.”
Preventive solutions for stent graft migration and leaks from the proximal seal zone include the experimental use of screw-type anchors to close the proximal seal. But to address type II endoleaks, a wholly novel approach is now being studied at Cleveland Clinic and other centers — one that could significantly cut the risk of endoleaks and stent migration in infrarenal stent grafts.
The investigational Nellix® EndoVascular Aneurysm Sealing System (Endologix) deploys twin catheters to the site of the infrarenal aneurysm. Balloons expand bilateral stents whose distal portions extend into the common iliac arteries. The stents are surrounded by endobags, which are pumped full of a fast-hardening biostable polymer. The polymer bags fill the aneurysmal sac and then anchor and seal the grafts —at the proximal end and at the bifurcation. The pressure of the endobags against the blood vessel walls seals off the opening of branches into the aneurysm sac, thus preventing type II endoleaks and limiting stent migration.
Advertisement
Placement of the system takes about 30 minutes and can be performed through a percutaneous approach.
The Nellix system can be used “out of the box.” Because it is able to accommodate a wider range of anatomies than can conventional EVAR, it holds the potential to expand the pool of patients who are eligible for endovascular AAA treatment.
Early studies suggest that the system may be able to drastically reduce the risk of late aneurysm rupture and decrease the need for secondary intervention or CT surveillance. An initial series of 34 patients in New Zealand demonstrated 100 percent technical success with the system, with no ruptures, endoleaks or need to convert to conventional repair.
Now a prospective multicenter trial — known as EVAS IDE — is underway to evaluate the safety and device performance of the Nellix system for the treatment of infrarenal AAAs. “Because this technology offers the possibility to completely mitigate endoleaks, patients may ultimately require less intense follow-up,” says Dr. Clair, who is site PI for the trial at Cleveland Clinic. “And the hope is that the long-term risk from these type II endoleaks may be eliminated.”
Enrollment in the EVAS IDE trial is ongoing at Cleveland Clinic; to refer a patient for trial evaluation, call 216.445.3608.
Advertisement
Advertisement

A sampling of outcome and volume data from our Heart & Vascular Institute

Concomitant AF ablation and LAA occlusion strongly endorsed during elective heart surgery

Large retrospective study supports its addition to BAV repair toolbox at expert centers

Young age, solid tumor, high uptake on PET and KRAS mutation signal risk, suggest need for lobectomy

Surprise findings argue for caution about testosterone use in men at risk for fracture

Residual AR related to severe preoperative AR increases risk of progression, need for reoperation

Findings support emphasis on markers of frailty related to, but not dependent on, age

Provides option for patients previously deemed anatomically unsuitable