Locations:

Elimination of most sex-related differences maintained five years after protocol adoption

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/74744e94-e98f-4f4f-9639-bf0c07eb2076/21-HVI-2284710-Hero-Option1-650x450-1_jpg)
21-HVI-2284710-Hero-Option1-650×450
The answer to closing the gender gap in the management of ST-elevation myocardial infarction (STEMI) may lie in adopting a comprehensive STEMI protocol, suggests a new analysis out of Cleveland Clinic.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
The observational cohort study, published online in European Heart Journal Open, found reduced sex disparities in various STEMI outcomes and quality measures through five years after implementation of Cleveland Clinic’s comprehensive protocol for STEMI management compared with the period before implementation.
“Sex disparities in STEMI care and outcomes have been widely reported, prompting the American Heart Association and the European Society of Cardiology to identify their reduction as a public health priority,” says the study’s corresponding author, Umesh Khot, MD, Head of Regional Cardiovascular Medicine at Cleveland Clinic. “Our study is the first to show how a systems approach using a comprehensive STEMI protocol can reduce mortality in women and largely eliminate disparities in death and other cardiovascular outcomes over a five-year period.”
Considerable literature evidence has demonstrated that, compared with their male counterparts, women with STEMI receive guideline-directed medical therapy less often and have a significantly longer average door-to-balloon time. These care disparities have resulted in significantly higher rates of in-hospital adverse events, new-onset heart failure and mortality from STEMI among women compared with men.
In July 2014, Cleveland Clinic adopted a four-step protocol designed to reduce variability in STEMI management across its facilities in Northeast Ohio. Soon afterward, it noticed that care metrics and outcomes improved across the board — but were particularly improved among female patients, thereby shrinking the traditional sex-based STEMI care gap.
Advertisement
Those results, published in the Journal of the American College of Cardiology (2018;71:2122-2132), were attributed to the new four-step protocol, which (as detailed in a prior Consult QD article) involved the following:
“Two years after implementing this comprehensive STEMI protocol, we observed improvements in use of guideline-directed therapy, door-to-balloon time and 30-day mortality in both sexes, but the improvements were especially pronounced in women, to the point that there were no longer statistically significant differences between the sexes,” says co-investigator Samir Kapadia, MD, Chair of Cardiovascular Medicine at Cleveland Clinic. “However, it was unclear whether these results could be consistently sustained over the long term.”
To explore that question, the researchers revisited results five years after implementation of the STEMI protocol. Their pre/post analysis assessed the management and outcomes of 1,833 consecutive patients with STEMI — 723 in the 3.5 years prior to protocol implementation (control group) and 1,110 in the five years following protocol implementation (protocol group). Women made up a similar share of the sample in the control and protocol groups (32.2% and 32.5%, respectively), and differences between men and women were consistent across the two groups.
Advertisement
The table below presents differences in process metrics and outcomes between male and female patients before and after the STEMI protocol. Prior to protocol implementation, results significantly favored males over females on all measures except for use of trans-radial PCI. In contrast, after protocol adoption, differences between the sexes were reduced to nonsignificant levels on all measures except for use of trans-radial PCI, which favored men, and net adverse clinical events, which trended toward favoring men. The latter outcome was largely attributable to a significantly higher rate of bleeding in female patients.
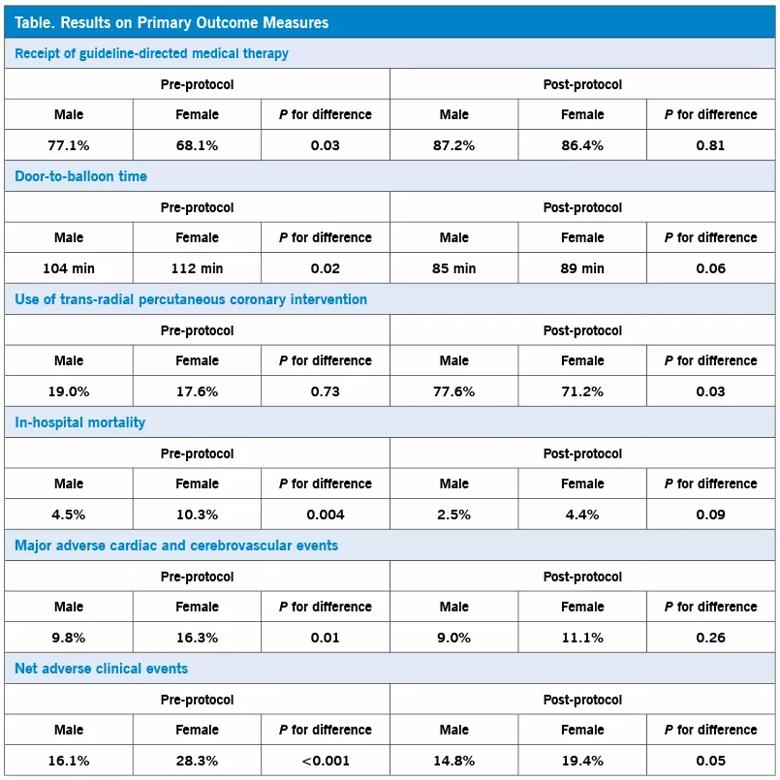
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/73a76d0f-3856-4f92-a18b-f7e257e870b9/21-HVI-2284710-Table-Inset-805x805-1_jpg)
“We have shown that door-to-balloon times and use of guideline-directed medical therapy were similar between the sexes for five years following adoption of our STEMI protocol,” says study co-author Grant Reed, MD, MSc, Director of Cleveland Clinic’s STEMI Program. “This corresponded to elimination of significant disparities in mortality and major adverse cardiac and cerebrovascular events between the sexes, although an excess of bleeding in women persisted. Use of trans-radial PCI also increased dramatically across the board with protocol implementation, although use in women still falls short of that in men.”
The authors note that their STEMI protocol differs fundamentally from other STEMI protocols that focus strictly on door-to-balloon time. “The Cleveland Clinic protocol is unique in its focus on early antithrombotic and antiplatelet drugs before PCI,” explains Dr. Kapadia. “Inappropriate variability in this area was minimized by our standardized STEMI checklist in the emergency department.”
Advertisement
“Maintaining early quality gains over the long term is a perennial challenge in hospital quality improvement efforts,” notes Dr. Khot. “That’s why these five-year results are reassuring.” He and his co-authors identify four reasons for the protocol’s enduring success:
“Although every health system is different,” Dr. Khot concludes, “we hope the sustained success of this protocol may serve as a model for others looking to improve their STEMI processes and outcomes and make substantial progress in closing the gender gap in STEMI care.”
Advertisement
Advertisement

A sampling of outcome and volume data from our Heart & Vascular Institute

Concomitant AF ablation and LAA occlusion strongly endorsed during elective heart surgery

Large retrospective study supports its addition to BAV repair toolbox at expert centers

Young age, solid tumor, high uptake on PET and KRAS mutation signal risk, suggest need for lobectomy

Surprise findings argue for caution about testosterone use in men at risk for fracture

Residual AR related to severe preoperative AR increases risk of progression, need for reoperation

Findings support emphasis on markers of frailty related to, but not dependent on, age

Provides option for patients previously deemed anatomically unsuitable