Locations:

New device looks to be a vital second-line therapy for selected patients
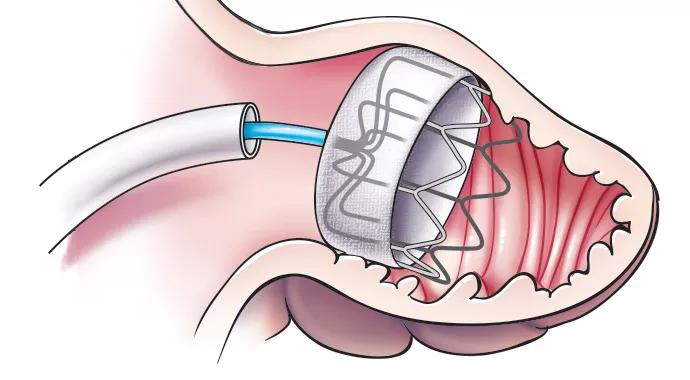
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/878a5f76-ebb4-4a43-aa18-c6b0bb615631/Watchman-690x380_jpg)
Watchman-690×380
The left atrial appendage (LAA) has been called “our most lethal human attachment,” but you’d never guess it from appearances: The LAA is a modest hollow sac that hangs from the left atrium, filling with blood and emptying along with the atrium. Its lethal reputation derives from the fact that in the 15 percent of patients with atrial fibrillation (AF) who suffer strokes, 90 percent of the culprit emboli are believed to originate in the LAA (see sidebar).
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
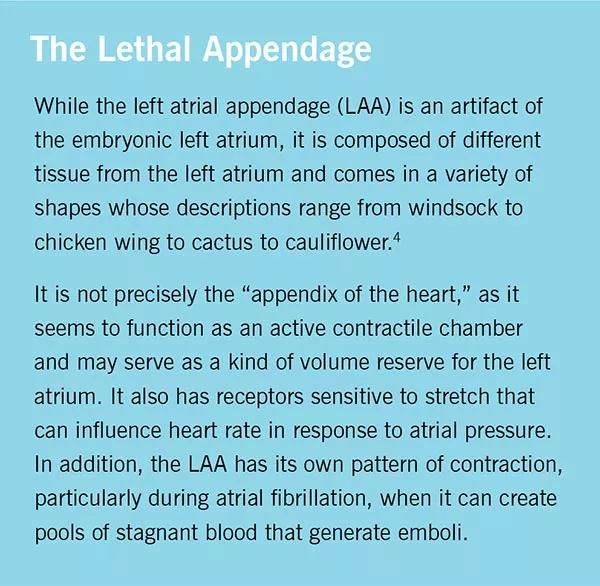
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/1909a6a7-967c-4cda-bbc2-553e56131f90/Watchman-inset-3_jpg)
The first-line treatment for stroke prevention in patients with nonvalvular AF remains warfarin despite its reputation as a high-maintenance anticoagulant with numerous food and drug interactions and the need for frequent monitoring to avoid gastric or cranial bleeding. Large numbers of patients who are prescribed warfarin cease to use it within a year, and it is contraindicated in many others.
The demand for alternatives to warfarin has brought about a wave of new oral anticoagulants in the past five years. Although these agents — direct thrombin inhibitors or direct factor Xa inhibitors — are useful for certain subgroups of patients, none yet seriously threatens warfarin’s dominance, in part because of their higher costs and their lack of an antidote to reverse active bleeding.
The ostium of the LAA has long been a tempting target to innovators seeking a nonpharmacologic alternative to warfarin. The LAA can be surgically removed, sutured, stapled or clipped closed during open surgery, with differing degrees of efficacy. Less invasively, several catheter-delivered devices for occluding the LAA have been developed and have undergone various degrees of testing.
In March 2015, after many years of review, the FDA approved the percutaneously implanted WATCHMAN™ Left Atrial Appendage Closure Device (Boston Scientific) for stroke risk reduction in patients with nonvalvular AF.
“WATCHMAN is a big development,” says Oussama Wazni, MD, Co-Director of the Ventricular Arrhythmia Center and Director of Outpatient Electrophysiology at Cleveland Clinic. “It’s implanted via a simple catheter-based procedure, and if there’s a good seal, there’s a very high likelihood the patient can be taken off oral anticoagulants.”
Advertisement
The WATCHMAN device is implanted in an interventional lab, under fluoroscopy. Transesophageal echocardiography (TEE) is used to assess the size and shape of the LAA.
During the procedure, a guidewire catheter is advanced through the femoral vein to the heart, where it is passed through a transseptal puncture to the left atrium (Figure 1). An access sheath and dilator are advanced into the left atrium, and a pigtail catheter is advanced into the LAA. In the final step, the device is inserted through the access sheath and aligned with the neck of the LAA. Once in position, the device is opened like a bulbous umbrella. Its flexible, fabric-covered nitinol frame conforms to the shape of the LAA (Figure 2).
| Figure 1. The transvenous, transseptal approach used for implantation of the WATCHMAN device in the LAA (upper right). Illustration reprinted from Cleveland Clinic Journal of Medicine (2015;82:167-176). | Figure 2. The WATCHMAN device opens like an umbrella to conform to the shape of the LAA. Illustration reprinted from Cleveland Clinic Journal of Medicine (2015;82:167-176). |
|---|---|
| Figure 1. The transvenous, transseptal approach used for implantation of the WATCHMAN device in the LAA (upper right). Illustration reprinted from Cleveland Clinic Journal of Medicine (2015;82:167-176). |
The procedure takes about an hour. The patient may go home the next day. Over the next several months, tissue overgrows the plug.
WATCHMAN has been commercially available in Europe since 2005 and is the leading percutaneous LAA closure device worldwide, with more than 10,000 patients having been treated.
Its U.S. approval was based on two major clinical trials, PROTECT AF and PREVAIL. The aggregate of both trials showed the device to be noninferior to warfarin in reducing the rate of stroke from any cause.
Several Cleveland Clinic investigators participated in these studies, including Dr. Wazni and fellow electrophysiologist Walid Saliba, MD, Medical Director of the Center for Atrial Fibrillation, as well as Samir Kapadia, MD, Director of the Sones Cardiac Catheterization Laboratory, and fellow interventional cardiologist Murat Tuzcu, MD, Vice Chair of the Department of Cardiovascular Medicine.
Advertisement
Drs. Kapadia and Tuzcu likewise published a systematic review and analysis of relevant observational studies that echoed these results, concluding: “Percutaneous LAA occlusion for stroke prophylaxis was comparable to historical controls for adjusted-dose warfarin and comparable to other anticoagulation agents.” These physicians also teamed with Dr. Saliba and interventional cardiology colleague Amar Krishnaswamy, MD, to publish a method for using CT-based imaging to potentially help plan the LAA occlusion procedure. TEE and CT scan are complementary for image guidance before and during the procedure.
The FDA has approved WATCHMAN for patients with nonvalvular AF who:
That indication gives physicians and patients considerable latitude for discussion. For Dr. Wazni, the “appropriate rationale” includes having a history of bleeding when taking oral anticoagulants or being deemed to have a high future risk of bleeding.
“WATCHMAN is a second-line therapy for a selected group of patients,” he says. “But for those patients, this is a very important option, as it can prevent stroke while avoiding the risk of bleeding.”
His colleague Dr. Saliba concurs, noting that patient preference looms large and additional experience should help refine decision-making. “It will take more education, more data and more time to see how it’s going to pan out,” Dr. Saliba says.
Advertisement
Dr. Kapadia adds: “Valvular AF refers to patients with rheumatic heart disease. As percutaneous treatment of valvular heart disease is expanding with transcatheter aortic valve replacement and the use of MitraClip®, many elderly patients with AF and nonrheumatic valvular heart disease can also benefit from this new advance.”
Advertisement
Advertisement

A sampling of outcome and volume data from our Heart & Vascular Institute

Concomitant AF ablation and LAA occlusion strongly endorsed during elective heart surgery

Large retrospective study supports its addition to BAV repair toolbox at expert centers

Young age, solid tumor, high uptake on PET and KRAS mutation signal risk, suggest need for lobectomy

Surprise findings argue for caution about testosterone use in men at risk for fracture

Residual AR related to severe preoperative AR increases risk of progression, need for reoperation

Findings support emphasis on markers of frailty related to, but not dependent on, age

Provides option for patients previously deemed anatomically unsuitable