Locations:

Often used for failed back surgery and complex regional pain syndromes

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/6edba9a8-7fa8-4834-b908-62e37998ca38/15-NEU-568-SpinalStim-690x380_jpg)
15-NEU-568-SpinalStim-690×380
By Andre Machado, MD, PhD; and Sean Nagel, MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
As shown by an increasing body of research, spinal cord stimulation (SCS) is a safe, efficacious, cost-effective and reversible treatment for select patients with severe chronic neuropathic pain.
SCS employs implanted epidural electrodes that deliver short-duration current or voltage pulses to excite sensory axons in the dorsal column. The precise mechanism of action of SCS remains unclear, and our understanding of chronic pain is incomplete. However, SCS is capable of interfering with the relay of non-nociceptive signals from the pain source, replacing painful sensation with more tolerable paresthesia and providing clinical improvement for some intractable pain syndromes affecting the extremities, with or without back involvement.
In the United States, SCS is most frequently used in cases of failed back surgery syndrome (FBSS) and complex regional pain syndrome (CRPS). SCS can alleviate axial and radicular pain, but is especially effective for patients with pain predominantly in the leg or arm. At Cleveland Clinic’s Center for Neurological Restoration, we have found the best candidates for this treatment generally are patients who experience persistent pain with neuropathic characteristics (often described as burning or aching), despite having undergone adequate decompressive surgery or spinal fusion.
The SCS system consists of one or more electrode leads connected to an implanted pulse generator similar to a pacemaker. We prefer to use rechargeable generators because of their longevity. Recharging is done at home — from several times per week to biweekly depending on battery size and individual patient electrical settings — by placing a charging device on the skin over the generator.
Advertisement
The SCS electrical leads, configured with four to 16 electrodes, are either cylindrical or paddle-shaped and are differentiated by their method of placement. Cylindrical (percutaneous) leads are implanted into the epidural space using large Tuohy needles, while paddle leads require a laminectomy or laminotomy. Though percutaneous leads are less invasive, paddle leads often are preferred because they are less prone to migrate and provide more efficient stimulation of the spinal cord.
Placement of the leads depends on the topography of the patient’s chronic pain. They are typically implanted in the mid or lower thoracic spine for patients with leg pain (with or without back pain), and in the middle or upper cervical areas for those with upper extremity pain.
Most patients undergo a psychological evaluation to help assess the probability of a successful outcome. Patients also undergo a test of the stimulation for one week with one or more externalized, percutaneously implanted leads connected to a pulse generator to determine the degree of analgesia and to assess if the patient tolerates stimulation well. A satisfactory response — generally a 50 percent or greater reduction in pain — is usually followed by permanent implantation.
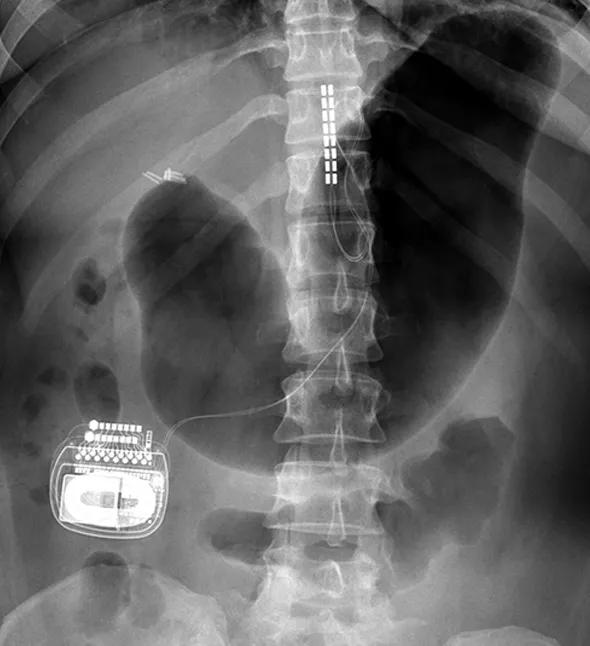
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/3c179500-fb49-4c47-854d-2f5130c0357d/15-NEU-568-SpinalStim-Inset_jpg)
Our experience in the Center for Neurological Restoration indicates that SCS’ effects seem to be long-lasting, as is patient satisfaction.
In 2011, we reported the results of a study evaluating the long-term outcomes of patients implanted with paddle lead SCS systems for FBSS or CRPS at our center between 1997 and 2008. The study assessed overall satisfaction with the therapy and correlated satisfaction with pain alleviation. We accomplished this by a retrospective chart review and a questionnaire survey to gauge present efficacy. We calculated pain reduction using pre- and postoperative scores on an 11-point visual analog scale (VAS). We also asked patients if they would undergo SCS implantation again if they were to have the same outcome.
Advertisement
Thirty-five patients participated in the study. More than 50 percent of those with CRPS reported greater than 50 percent pain relief at a mean follow-up of 4.4 years. Approximately 30 percent of the FBSS patients reported a 50 percent or greater improvement at a mean follow up of 3.8 years. Seventy-eight percent of patients with CRPS and 71 percent of patients with FBSS indicated they would undergo SCS surgery again for the same outcome. This disproportionately high degree of satisfaction suggests the VAS may not be the best way to measure long-term outcomes in these patients, and that improvements in quality of life may not be captured by this simplistic metric.
Our research found that patients implanted recently with SCS leads reported greater pain relief than those whose surgeries were earlier in the study period. This could represent a true decline in SCS efficacy over time, or alternatively may reflect the improvements in newer SCS equipment, with multichannel paddle leads and more programming features that may produce better outcomes than older systems.
At the Center for Neurological Restoration, we routinely implant SCS systems in patients with FBSS, CRPS and other chronic pain conditions. Our primary goal is to reduce pain-related disability and enable patients to be as active as possible. Our pain neuromodulation program has two specialized neurosurgeons and two full-time physician assistants. We strongly believe in a multidisciplinary approach to these complex disorders, and we routinely team with primary care, pain management, and physical medicine and rehabilitation physicians to provide long-term care. The best outcomes are likely achieved by pairing SCS with long-term physical therapy and rehabilitation.
Advertisement
Performed appropriately and in properly selected patients, SCS can be an effective therapy for managing refractory pain. Like other treatment options, however, it is not curative and should be combined with other modalities, especially physical therapy.
Dr. Machado is Director of Cleveland Clinic’s Center for Neurological Restoration. Dr. Nagel is an associate staff member of the Center for Neurological Restoration.
Advertisement
Advertisement

New study advances understanding of patient-defined goals

Testing options and therapies are expanding for this poorly understood sleep disorder

Real-world claims data and tissue culture studies set the stage for randomized clinical testing

Digital subtraction angiography remains central to assessment of ‘benign’ PMSAH

Cleveland Clinic neuromuscular specialist shares insights on AI in his field and beyond

Findings challenge dogma that microglia are exclusively destructive regardless of location in brain

Neurology is especially well positioned for opportunities to enhance clinical care and medical training

New review distills insights from studies over the past decade