Locations:

Extra caution in order for this vulnerable population
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/c8e88fa2-8581-4d6e-8dda-793a01b69e31/15-NEU-2522-Mehra-650x450_jpg)
15-NEU-2522-Mehra-650×450
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Cleveland Clinic’s Sleep Disorders Center has developed a focus in the area of sleep-disordered breathing (SDB) and atrial fibrillation (AF), identifying a strong magnitude of association in large population-based studies published in 2006 and 2009. Our investigations have also explored the intersection of both conditions with obesity. Yet an enduring knowledge gap surrounds interrelationships among SDB, obesity and AF following cardiac surgery.
This gap prompted us to embark on collaboration with Cleveland Clinic’s Miller Family Heart & Vascular Institute to examine the interrelationships of SDB, obesity and post-cardiac surgery AF. We share here an overview of our study rationale and findings.
SDB, which encompasses both obstructive and central sleep apnea, is characterized by repetitive upper airway collapse or cessation of breathing that is either complete (resulting in apneas) or partial (resulting in hypopneas). These sleep-related respiratory events are accompanied by intermittent bouts of hypoxemia, hypercapnia, autonomic dysregulation and intrathoracic pressure swings, leading to long-term adverse cardiovascular sequelae.
Our group has documented twofold to fourfold higher odds of AF in patients with a severe degree of SDB relative to those without SDB. We have also demonstrated an immediacy to the relationship of respiratory events with discrete arrhythmic events such as paroxysms of AF. These findings suggest an acute impact of the physiology of SDB superimposed on the likely chronic adverse influences of SDB pathophysiology in terms of cardiac remodeling. The result is creation of the ideal milieu for atrial arrhythmogenesis (Figure 1).
Advertisement
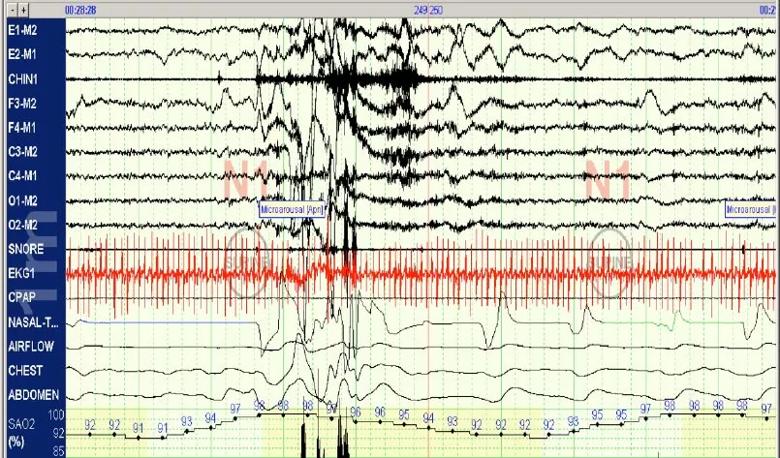
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/0c7c7ead-dcf1-4243-98d8-ec9f479a83f7/15-NEU-2522-Inset-1_jpg)
Figure 1. Polysomnogram in a patient with atrial fibrillation demonstrating an obstructive apnea (blue tracing and arrow) and a hypopnea (green tracing and arrow) with accompanying oxygen desaturations and an EEG microarousal.
Although obesity is a recognized risk factor for both SDB and AF, parsing out the complex and multidirectional relationships of SDB and obesity in relation to cardiac outcomes remains a substantial challenge, as detailed by a recent Heart Rhythm Society research forum. In addition to an increase in parapharyngeal fat pads resulting from obesity-related mechanical load, leptin resistance and an increase in systemic inflammation may also represent risks for SDB.
Bidirectional relationships are likely at play, with pathways of metabolic dysregulation and insulin resistance that may represent intermediate factors contributing to obesity in SDB. Additionally, the literature has increasingly implicated obesity in AF development, likely via pathophysiologic mechanisms related to genetic susceptibilities, coronary artery disease, ventricular adaptation and visceral/epicardial adiposity leading to cardiac electrical and structural remodeling.
The prevalence of AF following cardiac surgery is high: 33 percent among patients undergoing coronary artery bypass graft surgery (CABG) and 50 percent among those having valvular surgery. Identification of risk factors is key, as post-cardiac surgery AF portends a poor prognosis and is associated with adverse outcomes including increased rates of postoperative stroke, increased hospital stay and healthcare costs, and a trend toward lower survival.
Advertisement
Despite the substantial impact of post-cardiac surgery AF, studies to date have been limited by at least three factors:
Our collaborative study with the Miller Family Heart & Vascular Institute set out to address these limitations by examining the interrelationships of SDB, obesity and post-cardiac surgery AF among patients who underwent both cardiac surgery (CABG and/or valvular surgery) and polysomnography within three years of each other at Cleveland Clinic from 2009 to 2014. We restricted the study to patients 18 or older without known AF or atrial flutter, which yielded a sample of 190 patients.
SDB was defined by the apnea-hypopnea index (AHI), using the 3 percent oxygen desaturation scoring rule, or alternately by the oxygen desaturation index. Indices to characterize obstructive sleep apnea (obstructive apnea-hypopnea index) and central sleep apnea (central apnea index) were also examined.
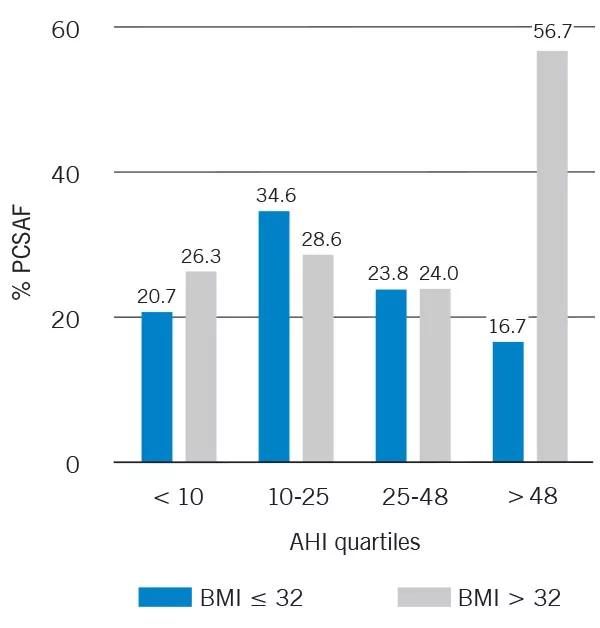
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/662b6fcd-781c-440c-82f7-81720f3cf147/15-NEU-2522-Inset-2_jpg)
Figure 2. Graph showing rates of post-cardiac surgery atrial fibrillation (PCSAF) by apnea-hypopnea index (AHI) quartiles and stratified by median BMI (N = 190).
Overall, the patient sample was relatively old (60.6 ± 11.4 years) and obese (BMI of 33.3 ± 7.5 kg/m2). Ninety-three percent of patients had an AHI of 5 or greater, and the prevalence of postoperative AF was 30 percent, in line with existing reports.
Advertisement
We identified a statistically significant association of postoperative AF with AHI-defined SDB but not specifically with obstructive or central sleep apnea. After adjusting for obesity and other confounders, the relationship was slightly attenuated. Notably, obesity was found to be an effect modifier of the relationship, in that SDB was more closely associated with post-cardiac surgery AF in those who were more obese, a finding particularly pronounced in patients with the most severe degree of SDB (Figure 2).
These findings were highlighted as a platform presentation at SLEEP 2015, the annual meeting of the Associated Professional Sleep Societies, and are being submitted for publication. They are important because they suggest that patients with both SDB and obesity may represent a particularly vulnerable group that merits targeting to reduce post-cardiac surgery AF and its attendant morbidity.
These findings also serve as a springboard for future investigations to examine their reproducibility in other patient populations, to enhance understanding of the mechanisms by which SDB and obesity may operate together to increase AF risk following cardiac surgery, and to evaluate the effectiveness of interventions targeted at SDB and obesity to reduce post-cardiac surgery AF.
Dr. Mehra is Director of Sleep Disorders Research in the Sleep Disorders Center in Cleveland Clinic’s Neurological Institute. She also has appointments in the Respiratory Institute, the Miller Family Heart & Vascular Institute and the Lerner Research Institute’s Department of Molecular Cardiology.
Advertisement
Advertisement

A sampling of outcome and volume data from our Heart & Vascular Institute

Concomitant AF ablation and LAA occlusion strongly endorsed during elective heart surgery

Large retrospective study supports its addition to BAV repair toolbox at expert centers

Young age, solid tumor, high uptake on PET and KRAS mutation signal risk, suggest need for lobectomy

Surprise findings argue for caution about testosterone use in men at risk for fracture

Residual AR related to severe preoperative AR increases risk of progression, need for reoperation

Findings support emphasis on markers of frailty related to, but not dependent on, age

Provides option for patients previously deemed anatomically unsuitable