Locations:

Severe pain and ulceration affecting fingertips

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/7ca69801-463f-48f2-a30a-b6d62f0b112f/19-RHE-1387-ulcerationFingertips-650x450_jpg)
19-RHE-1387-ulcerationFingertips-650×450
By Soumya Chatterjee, MD, MS, FRCP
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
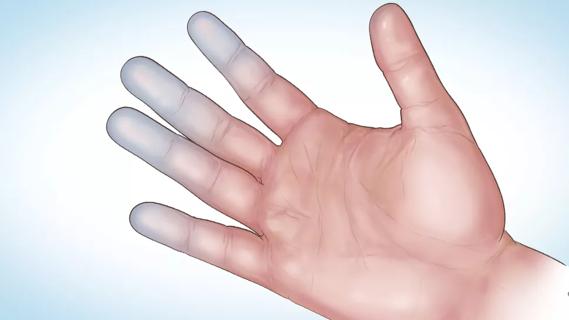
A 58‐year‐old female with an 18‐year history of limited cutaneous systemic sclerosis presented with severe pain and ulceration affecting the tips of her fingers.
On examination, there was evidence of auto‐amputation of some of her distal phalanges and ulceration of the overlying skin.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/4cf52387-a37d-4c34-a59a-6e91e9dac0a6/Panel-A-1-300x225_jpg)

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/8217f947-ffa3-46de-b1d9-c0a06854c73f/Panel-A-2-300x225_jpg)

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/1e79872b-4b5f-459b-a21c-d11303b1c0fd/Panel-A-3-300x225_jpg)
Hand radiographs demonstrated resorption of the first and fourth distal phalanges as well as the second, third, and fifth middle phalanges of the right hand, in addition to resorption of the first, second, fourth, and fifth distal phalanges as well as the third middle phalanx of the left hand (acro‐osteolysis), along with resorption of overlying soft tissues.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/c83b315c-6891-48cb-8db4-9b81929ffd24/Panel-B-300x221_jpeg)
These changes had developed insidiously because of severe persistent digital ischemia associated with systemic sclerosis.
The patient did not get maximum pain relief with trials of various oral vasodilators, such as calcium channel blockers, alpha‐blockers, losartan, pentoxifylline, phosphodiesterase‐5 inhibitors and topical nitroglycerin. Intravenous prostaglandin analogs — such as prostacyclin, alprostadil and treprostinil — are useful for the treatment of severe digital ischemia in systemic sclerosis. Thus, she was admitted for a 5‐day course of continuous intravenous alprostadil infusion, which was chosen for its ease of use and lower price.1 It provided substantial pain relief lasting for several months.
Acro‐osteolysis associated with a diverse group of illnesses, such as scleroderma spectrum disorders, psoriasis, hyperparathyroidism, diabetes mellitus, leprosy, thermal burns, frostbite and chronic polyvinyl chloride exposure. It can also occur in rare genetic disorders such as progeria, pyknodysostosis and Hajdu‐Cheney syndrome.
Advertisement
Acro‐osteolysis is rare; however, it is estimated to occur in about 20% to 25% of patients with systemic sclerosis.2,3 It is believed to result primarily from hypoxia‐induced upregulation of vascular endothelial growth factor, leading to increased osteoclastogenesis and enhanced osteoclastic bone resorption.4 However, although acro‐osteolysis is assumed to result from critical digital ischemia, it often develops even without digital ulcers, indicating that other factors may also play an essential role in its pathogenesis.4
Systemic sclerosis is an autoimmune disease of unclear etiology characterized by progressive fibrosis of skin and various internal organs (mainly the lungs, heart, gastrointestinal tract and kidneys), a widespread occlusive microvasculopathy and presence of certain autoantibodies.
Advertisement
Please note: This article is a revised version of the work that was originally published in ACR Open Rheumatology, and is reused in accordance with the Creative commons Attribution-NonCommercial License. The work was originally published as: Chatterjee S. Clinical image: Acro-osteolysis. ACR Open Rheumatology. 2019 Aug 25. https://doi.org/10.1002/acr2.11072
Dr. Chatterjee directs the Scleroderma Program in the Department of Rheumatic and Immunologic Diseases.
Advertisement
Advertisement
Treatment strategies require understanding of pathomechanisms

Education, prevention strategies and monitoring serves this at-risk group

Treatment for scleroderma can sometimes cause esophageal symptoms

Lupus Clinic providers collaborate to advance treatment and understanding

Older Psoriasis Patients May Experience Quicker Transition

Cleveland Clinic’s Rheumatic Lung Disease program treats patients with complex conditions

Symptoms complement one another

E-coaching program is tailored for those with the disease