Locations:

Should complete hemispherectomy be considered for this infant?
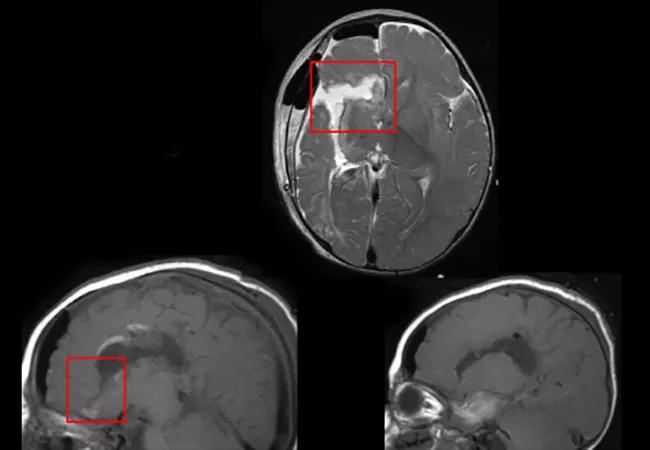
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/0e2eb4bd-bb57-4381-b3a3-cd69ceef587f/16-NEU-1992-Binagman-650x450_jpg)
16-neu-1992-binagman-650×450
By William Bingaman, MD, and Elaine Wyllie, MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Ten-month-old “Laurie” presents with daily seizures, hemiparesis (left hand fisting) and developmental delay (no smiling and inability to roll over or sit). Her parents first noted seizures at age 3 months; these consist of clusters of left or bilateral spasms and arrest of activity, during which her eyes turn to the left. Trials of seven antiepileptic medications, including pyridoxine, have not helped.
Her perinatal course was marked by preeclampsia, decreased fetal movement, reduced heart rate and premature birth. MRI subsequently revealed that she had suffered a perinatal right middle cerebral artery (MCA) infarction, with extensive cystic encephalomalacia. The images also showed subtle focal abnormality in the left frontal lobe, consistent with gliosis.
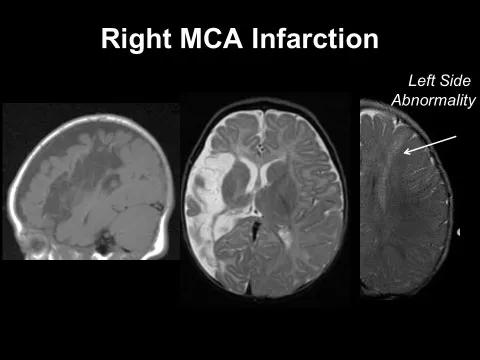
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/023f2b09-4b5e-438e-8733-c0d0ce98396f/16-NEU-1992-Binagman-Inset-1_jpg)
At 10 months, her EEG shows hypsarrhythmia, with abundant high-amplitude spikes bilaterally as well as runs of spikes localized to the right posterior temporoparietal region. EEG seizures are nonlocalized.
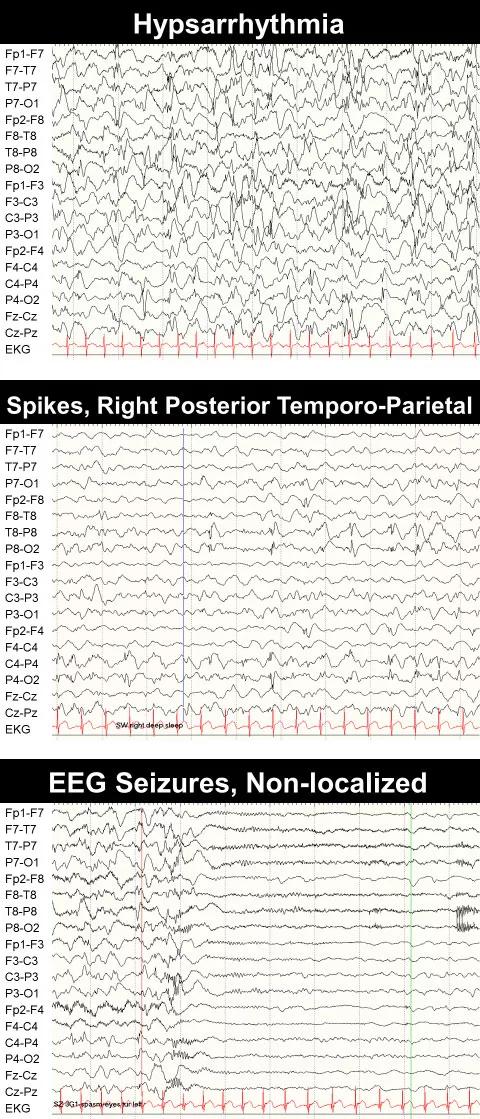
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/4514af05-1e45-4600-8915-20e781bb5e7c/16-NEU-1992-Binagman-Inset-2_jpg)
Although EEG shows widespread seizure activity, all data must be considered, especially for a young child. The focal EEG spikes in the right temporoparietal region, together with the right MCA infarction, suggest that her seizures resulted from the injury to that hemisphere.
Based experience in similar cases, Laurie appears to be a favorable candidate for right disconnective hemispherectomy, despite the bilateral findings on EEG and MRI. Research shows that outcome is not significantly affected by the presence of a less-severe contralateral abnormality on preoperative MRI, which can actually be found in 75 percent of patients who undergo hemispherectomy. Since the status quo is clearly catastrophic for this child, the team recommends surgery.
Advertisement
A right disconnective (“functional”) hemispherectomy is performed, in which the connections between the hemispheres are severed but the hemisphere left in place. No immediate complications are evident.
On postoperative day 4, the parents note staring again, but now with eye deviation to the right. This may have a benign explanation: It is not uncommon to see unusual behaviors following hemispherectomy. But because concern has been raised, further investigations are pursued.
EEG now shows clear asymmetry, with all rhythms markedly reduced on the operated right side. She now has unilateral or hemi-hypsarrhythmia on the left — and only a few isolated spikes on the right. Furthermore, the ictal EEG patterns are also higher on the left, with an initial high-amplitude sharp wave followed by paroxysmal fast activity.
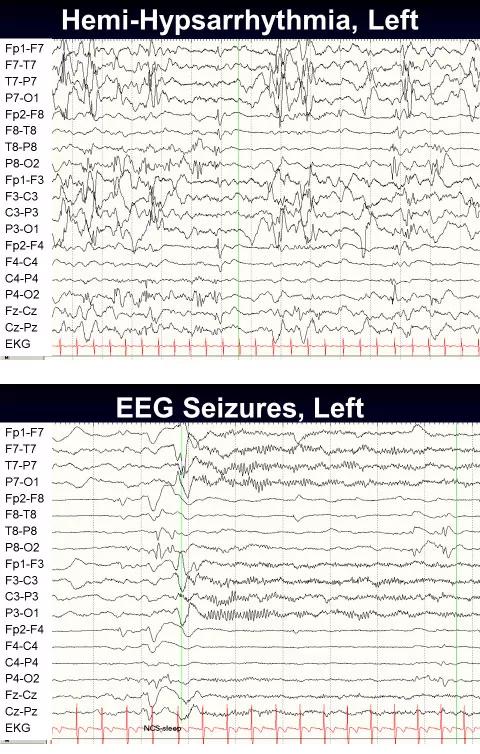
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/002bba66-c911-4a87-af48-44dc5c8fb4ab/16-NEU-1992-Binagman-Inset-3_jpg)
Interpreting post-hemispherectomy EEGs is challenging. Seizures may arise within focal areas of the operated side and then propagate to the contralateral side, where they show up on EEG. It is possible that her disconnection is incomplete, even though this is not apparent on MRI.
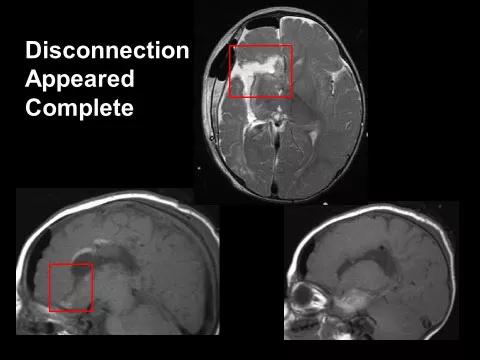
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/f55bffcf-f13c-4158-9cc7-564f0ba750a7/16-NEU-1992-Binagman-Inset-4_jpg)
Despite the diagnostic challenges, complete (“anatomical”) hemispherectomy should be considered for continued seizures after a disconnective hemispherectomy, even if the side of seizure onset cannot be confirmed with EEG or MRI. EEG may show spread patterns on the contralateral side, and MRI may fail to reveal small nests of connected epileptogenic neurons.
In our experience, complete hemispherectomy following disconnective hemispherectomy leads to freedom from seizures in about half of cases and to worthwhile improvement in another quarter. Complete hemispherectomy entails the risk for hydrocephalus requiring shunting, and children must be followed even after successful surgery.
Advertisement
In our case, although the side of seizure onset is impossible to determine with certainty based on the available evidence, it is decided to proceed with a complete hemispherectomy, allowing confidence that no residual tissue will remain in the right hemisphere.
Six months postoperatively, Laurie has been seizure-free and her EEG shows normal rhythms on the left side. The hemi-hypsarrhythmia has completely resolved.
This case highlights medical and ethical issues in deciding whether to perform surgery in the face of significant unknowns. One must keep in mind that for patients with persistent seizures after disconnective hemispherectomy, complete hemispherectomy may be beneficial even if EEG and MRI do not confirm the side of seizure onset. Educating parents to make informed decisions is imperative.
To view a webcast of this and nine other epilepsy cases in the “Hot Topics in Epilepsy for Children and Adults” CME-certified webcast series, visit ccfcme.org/EpilepsyCME. This activity has been approved for AMA PRA Category 1 Credit™.
Dr. Bingaman is Vice Chairman of Cleveland Clinic’s Neurological Institute and Head of the Section of Epilepsy Surgery.
Dr. Wyllie is a professor at Cleveland Clinic Lerner College of Medicine and a pediatric epilepsy specialist in Cleveland Clinic’s Epilepsy Center.
Advertisement
Advertisement

New study advances understanding of patient-defined goals

Testing options and therapies are expanding for this poorly understood sleep disorder

Real-world claims data and tissue culture studies set the stage for randomized clinical testing

Digital subtraction angiography remains central to assessment of ‘benign’ PMSAH

Cleveland Clinic neuromuscular specialist shares insights on AI in his field and beyond

Findings challenge dogma that microglia are exclusively destructive regardless of location in brain

Neurology is especially well positioned for opportunities to enhance clinical care and medical training

New review distills insights from studies over the past decade