Locations:

Early experience supports the approach in select patients

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/7ddf545e-14e8-471c-97fd-14e8b05d0184/seeg-690x380_jpg)
seeg-690×380
By Jorgé Gonzalez-Martinez, MD, PhD; Elaine Wyllie, MD; and Deepak Lachhwani, MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Subdural grids and strips are the most common invasive method used in the United States for pediatric epileptic patients who need extraoperative invasive monitoring procedures. Despite the high spatial resolution provided by the subdural methodology, which allows for accurate mapping of superficial cortical areas, relatively deep epileptic foci cannot be localized with adequate spatial and temporal resolution. Moreover, subdural grids require relatively large craniotomies and are generally limited to exploration of one hemisphere — important limiting factors in the pediatric population.
In search of a better way: SEEG methodology
In the face of these relative limitations, we explored alternative/complementary methods for invasive monitoring, revisiting the concepts and techniques of the stereoelectroencephalography (SEEG) methodology and applying it to a selected group of pediatric patients with difficult-to-localize epilepsy.
We recently published our early experience with SEEG for extraoperative mapping of difficult-to-localize refractory focal epilepsy. We focus here on results in the large cohort of pediatric and adolescent patients (n = 30) from that broader analysis.
Basics of the study design
We consecutively studied all pediatric patients (younger than 21 years) with the diagnosis of medically refractory focal epilepsy who underwent SEEG implantation at Cleveland Clinic’s Epilepsy Center between August 2009 and March 2012. All surgeries were part of standard patient care, and no procedures were performed for research purposes. Postoperative clinical data were collected by patient interview, during regularly scheduled clinic visits or by telephone.
Advertisement
Postoperative seizure outcome was classified according to the Engel Epilepsy Surgery Outcome Scale. All adverse events within 30 days after SEEG implantation were counted as complications.
Results: SEEG-guided resections
The hypothetical epileptogenic zone (EZ) was localized in 26 of 30 patients (86.6 percent). Of these patients, 18 (69.2 percent) underwent resection (Table 1). Reasons for not undergoing resection despite localization of the hypothetical EZ included failure in localizing the EZ (n = 4); multifocal EZ (n = 4); EZ localization in eloquent cortex, preventing resection (n = 3); and improvement of seizures after implantation (n = 1).
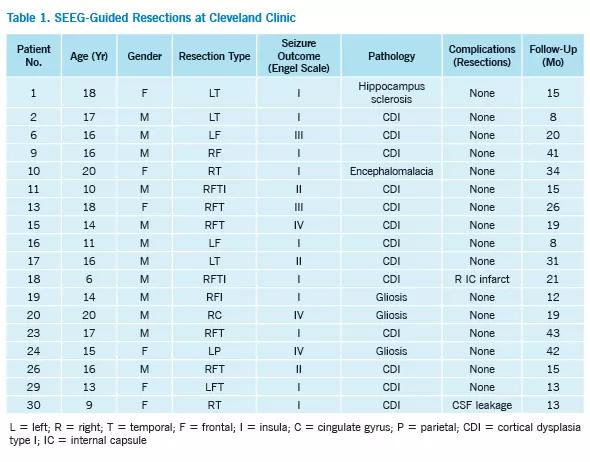
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/a7dd70b5-3418-4e6c-9536-406ed2c15b65/table-1_jpg)
The total number of implanted electrodes was 402 (average of 13.4 electrodes per patient). Each patient underwent two or three surgical procedures (12 and 18 patients, respectively), which included SEEG implantations, SEEG electrode removals and SEEG-guided resections. In total, 78 procedures were performed.
Among the 18 patients who underwent surgical resections, preoperative MRIs were nonlesional in 11 patients (61.1 percent). Eleven patients (61.1 percent) had resections on the right side, and seven (38.9 percent) on the left side. Temporal lobe resections were performed in five patients (27.7 percent), unilobar extratemporal resections in five (27.7 percent), and multilobar resections in eight (44.4 percent).
In the SEEG implantation series, no child experienced serious or permanent morbidity. One patient developed a small and asymptomatic intraparenchymal hematoma, which required no surgical intervention or prolonged hospital stay. The complication rate was 3.3 percent. The rate of hemorrhagic complications per implanted electrode was 0.2 percent. The average estimated blood loss per SEEG implantation procedure was 5 cc. The average hospital stay for the SEEG implantations was 9.7 days.
Advertisement
Results: Seizure outcomes and pathology
The mean follow-up after SEEG-guided resections was 21.9 months (range, 8 to 43). Of the 18 patients who underwent resection:
Figure 1 presents illustrative images from one of the patients who achieved seizure freedom.
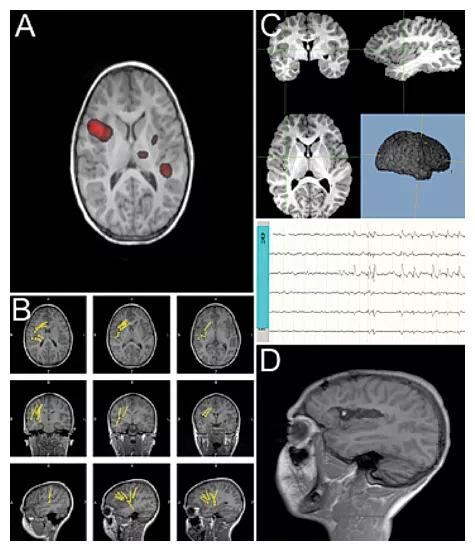
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/f9e3eb7c-18fc-45d3-9ebd-9d17d189b4de/figure-1_jpg)
Figure 1. Illustrative case of a 14-year-old male with medically intractable focal epilepsy for 12 years (patient 9 in Table 1). Multiple scalp EEGs showed multifocal epileptic discharges (temporal, frontal and parietal) on the right. MRI was considered nonlesional. (A) Ictal SPECT showing increased blood flow in the right frontal opercular and insular regions. (B) MEG scans showing dipoles located in the right frontal opercular areas. (C) SEEG implantation and co-registration with preoperative MRI demonstrating right frontal, perisylvian, insular, temporal and parietal SEEG implantation. On the bottom, SEEG ictal recordings demonstrate ictal onset in the R electrodes in contacts located in the superior insula and frontal opercular areas. (D) Postoperative MRI after SEEG-guided resection focused on the right superior insula and frontal opercular area. The patient has been seizure-free for 12 months.
Surgical pathology performed on specimens from the 18 patients who underwent resection showed:
Advertisement
Among the three patients with no seizure improvement, histopathology showed gliosis in two and a mild form of cortical dysplasia in the remaining patient (Table 1).
SEEG-guided resection: An additional opportunity for seizure freedom
We conclude that the SEEG method, when individualized through careful and meticulous analysis, is a safe and efficient option for pediatric patients who present with clinical features of medically intractable focal epilepsy in the setting of nonlocalizable scalp EEG recordings and with nonlesional MRIs.
In performing SEEG in this highly selected group, we were able to partially overcome the relative limitations of the current standard methods of invasive monitoring. This approach offers an additional opportunity for seizure freedom without safety compromises in clinically challenging cases — an opportunity likely not possible with other methods of extraoperative invasive monitoring.
Dr. Gonzalez-Martinez is a neurosurgeon specializing in pediatric epilepsy surgery and pediatric brain tumors. He is an associate staff member in Cleveland Clinic’s Epilepsy Center and the Departments of Neurological Surgery and Biomedical Engineering.
Dr. Wyllie is a professor and pediatric epileptologist in Cleveland Clinic’s Epilepsy Center.
Dr. Lachhwani is a pediatric epileptologist in Cleveland Clinic’s Epilepsy Center.
Advertisement
Advertisement

New study advances understanding of patient-defined goals

Testing options and therapies are expanding for this poorly understood sleep disorder

Real-world claims data and tissue culture studies set the stage for randomized clinical testing

Digital subtraction angiography remains central to assessment of ‘benign’ PMSAH

Cleveland Clinic neuromuscular specialist shares insights on AI in his field and beyond

Findings challenge dogma that microglia are exclusively destructive regardless of location in brain

Neurology is especially well positioned for opportunities to enhance clinical care and medical training

New review distills insights from studies over the past decade