Locations:

Investigating patient-specific bony anatomy, implant location and shoulder motion to avoid scapular notching
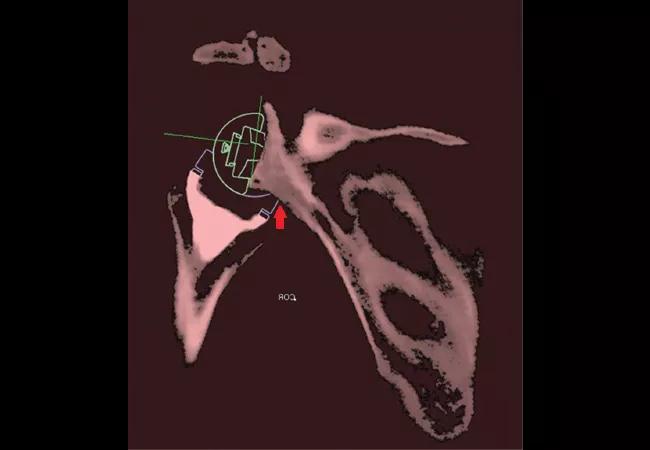
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/0d27ede9-5749-4534-9350-ca68382f74ba/17-ORT-1252-Ricchetti-Hero-Image-650x450pxl_jpg)
17-ORT-1252-Ricchetti-Hero-Image-650x450pxl
By Joel Kolmodin, MD; Iyooh U. Davidson, MD; Bong-Jae Jun, PhD; Nipun Sodhi, MD; Naveen Subhas, MD; Thomas Patterson, PhD; Zong-Ming Li, PhD; Joseph P. Iannotti, MD, PhD; and Eric T. Ricchetti, MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
In a recent study that we conducted of patients who underwent a reverse total shoulder arthroplasty (rTSA), we found that areas of bony impingement on shoulder range of motion (ROM) matched the areas of radiographic scapular notching that develop postoperatively. This relationship was demonstrated using 3-D computed tomography (CT) kinematic simulation of patients’ actual implant position from CT and actual postoperative ROM from video motion analysis (VMA). This connection between impingement and notching, while implied in prior studies, has not previously been directly shown in a clinical population.
Scapular notching is frequently observed following rTSA, although its etiology is not well-understood. It has been suggested that prosthesis design, scapular anatomy and implant position are responsible for this problem. Studies have used cadaver models, finite element analysis, computer modeling and retrospective radiographic review to examine either factors that influence impingement-free shoulder ROM following rTSA or factors associated with postoperative radiographic scapular notching. But the connection between impingement and notching has not been investigated directly.
The purpose of our study was to determine whether patient-specific postoperative shoulder ROM and bony impingement of the humeral component along the scapular neck on 3-D CT imaging analysis are predictive of the presence and location of radiographic notching that develops following rTSA. We also evaluated patient and prosthetic factors associated with scapular notching and changes in implant position needed to avoid patient-specific bony impingement.
Advertisement
Thirty patients with preoperative CT scans who underwent rTSA were evaluated at minimum two-year follow-up with VMA, postoperative 3-D CT with metal artifact reduction techniques and standard radiographs. Reflective markers were placed on each patient’s skin at specific bony prominences on the forearm, arm, scapula and thorax to perform VMA of patients’ shoulder ROM during active abduction/ adduction and internal rotation/external rotation with the arm at the side. Glenohumeral ROM was then determined for each patient from VMA. This information was then combined with postoperative implant location from 3-D CT in custom 3-D CT kinematic simulation software to determine areas of bony impingement between the humeral implant and scapula (Figure 1).
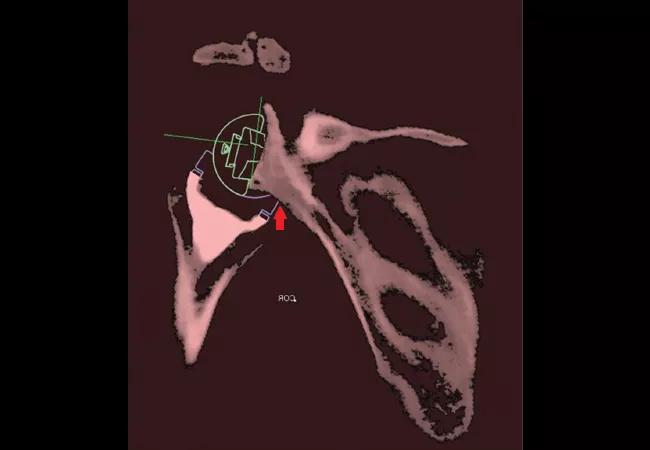
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/fef64a34-d13f-43d9-8202-9782d0168cb3/17-ORT-1252-Ricchetti-Inset-Image-01-650x450pxl_jpg)
Figure 1 Digital templates for the humeral and glenoid components were aligned with actual component positions on postoperative CT. Postoperative glenoid implant position was then registered to the preoperative CT using an image overlay technique available in the 3-D imaging software, such that the position and orientation of the glenoid component digital template on the postoperative scapula was transferred to the preoperative scapula, as shown in Figure 1. The postoperative humerus and the position and orientation of the humeral component digital template were mated to the preoperative scapula with postoperative glenoid component digital template as part of the overlay technique. During 3-D CT kinematic simulation of patients’ glenohumeral ROM, an automated detection method within the custom-designed 3-D imaging software detects impingement between the humeral component and the scapular neck, shown by the red arrow in the figure.
Advertisement
The presence of impingement was correlated with the presence of scapular notching on postoperative CT and plain radiographs. We also investigated translational (lateral, inferior and posterior) and rotational (version and inclination) modifications to glenosphere position that eliminated bony impingement.
Seventeen patients had evidence of scapular notching on CT and/or plain radiographs at a minimum two-year follow-up. All had evidence along the posteroinferior scapular neck (Figure 2) and three along the anteroinferior neck. Bony impingement was observed during 3-D CT kinematic simulation of patients’ glenohumeral ROM with external rotation and the arm at the side in 16 out of 17 patients, with internal rotation and the arm at the side in three of 17 patients, and with adduction and neutral rotation when moving through the abduction-adduction arc in 12 of 17 patients. The remaining 12 patients who underwent VMA did not have scapular notching or bony impingement. Bony impingement in the 3-D CT simulation was significantly associated with the presence of postoperative notching (P < 0.001), and the location of impingement matched the location of notching on postoperative CT in all patients.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/2a3f2731-90ea-44f7-9233-a493231862d4/17-ORT-1252-Ricchetti-Inset-Image-02-650x450pxl_jpg)
Figure 2 Evidence of scapular notching along the posteroinferior scapular neck, observed on a postoperative CT scan and shown by the red arrow, with the notched scapula outlined in yellow.
In evaluating factors associated with scapular notching, patients with notching had significantly greater preoperative glenoid retroversion (mean -17.4 ± 14.2° versus -7.7 ± 10.4°, P = 0.04) than patients without notching. Insufficient inferior (mean -0.3 ± 3.4 mm versus 2.8 ± 2.9 mm, P = 0.015) or posterior (mean -0.3 ± .5 mm versus 3.8 ± 2.6 mm, P = 0.002) glenosphere placement was also associated with scapular notching. On multivariate analysis, combined inferior and posterior (C-index 0.864, P = 0.0014) or inferior and lateral (C-index 0.860, P = 0.0015) glenosphere position was significantly different between the notching and non-notching groups. For patients’ given ROM, placing the glenosphere in a more inferior (mean 3.4 ± 2.3 mm) or lateral position (mean 6.2 ± 1.4 mm) would have most avoided impingement in those who demonstrated impingement on 3-D CT kinematic simulation.
Advertisement
Our results demonstrate the connection between bony impingement and postoperative radiographic scapular notching in patients who have undergone rTSA. Notching is a 3-D phenomenon that appears to develop from bony impingement along the posteroinferior scapular neck and occurs most commonly from external rotation with the arm at the side.
Inferior and/or lateral or posterior glenosphere placement was found to be an important factor for avoiding notching. While posterior glenosphere position, relative to inferior and lateral placement, has not been commonly discussed as important in avoiding notching, its importance is supported by the observation of the posteroinferior scapular neck being the most common site of notching and impingement.
Glenosphere position can be modified to avoid bony impingement with only small changes, suggesting that preoperative determination of ideal implant position based on patient specific bony anatomy and kinematic ROM criteria may be a helpful surgical planning tool to avoid notching postoperatively.
Drs. Kolmodin and Davidson are residents; Dr. Sodhi is a research fellow; Drs. Jun and Patterson are researchers; Dr. Subhas is on staff in the Radiology Department; Dr. Li is on staff in the Biomedical Engineering Department; Dr. Iannotti is Chairman, Orthopaedic & Rheumatologic Institute; and Dr. Ricchetti is staff in the Department of Orthopaedic Surgery.
Advertisement
Advertisement

Biologic approaches, growing implants and more

Study reports zero infections in nearly 300 patients

How to diagnose and treat crystalline arthropathy after knee replacement

Study finds that fracture and infection are rare

Center will coordinate, interpret and archive imaging data for all multicenter trials conducted by the foundation’s Osteoarthritis Clinical Trial Network

Reduced narcotic use is the latest on the list of robotic surgery advantages

Cleveland Clinic specialists offer annual refresher on upper extremity fundamentals

Cleveland Clinic orthopaedic surgeons share their best tips, most challenging cases and biggest misperceptions