Locations:

A rundown of what determines good and bad candidates

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/6bf56186-a676-4bd5-93a1-0b0780e6d475/RoboticHybrid-690x380_jpg)
Robotic surgical arm
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Hybrid coronary revascularization combines minimally invasive coronary artery bypass grafting (CABG) with a catheter-based intervention as an alternative to open CABG with sternotomy and percutaneous coronary intervention (PCI). The aim is to bring the most favorable aspects of both cardiac surgery and interventional cardiology to bear for patients with multivessel coronary artery disease.
The approach typically involves anastomosis of the left internal mammary artery (LIMA) to the left anterior descending (LAD) artery — the most durable aspect of CABG — in conjunction with stenting of non-LAD target lesions. When used in appropriate lesions, stents have been shown to provide long-term patency equivalent to that of vein grafts.
The surgical component of this approach can be offered either partially or entirely endoscopically using robotic technology, thereby avoiding sternotomy or large thoracotomy. However, hybrid revascularization is still in its infancy, with only about 1,200 reported cases performed nationwide. The procedure is restricted to a handful of medical centers where surgeons have mastered less-invasive CABG and have a close association with interventional cardiologists committed to the hybrid approach.
In the largest reported series of robotic hybrid revascularization procedures to date (N = 226), hospital mortality was 1.3 percent and the average length of stay was six days. Patients were able to resume normal household chores within 14 days and full activity at 42 days. Five years post-procedure, the survival rate was 92.9 percent and 75.2 percent of patients were free from major adverse cardiovascular events. In this series, 2.7 percent of the bypass grafts and 14.2 percent of PCI lesions required reintervention.
Advertisement
Hybrid revascularization has been performed at Cleveland Clinic for several years, generally with the surgical portion of the case performed first and the PCI procedure occurring at a separate time afterward.
We remain conservative, reserving the technique for patients with specific indications, as discussed further below.
Evaluation of a patient’s suitability for robotic hybrid revascularization is done by a team including interventional cardiologists and cardiothoracic surgeons specializing in robotically assisted procedures. All team members must understand the benefits and limitations of the procedure. Our overarching goal is to offer every patient the best procedure for his or her individual case. When considering hybrid revascularization, we seek to ensure the technique will provide revascularization quality equivalent to that of open CABG.
Although patients at high risk from CABG are often referred for hybrid revascularization, the robotic approach is not necessarily less risky than open revascularization. Complicated patients with widespread disease are not amenable to stenting. Patients with a low ejection fraction and comorbidities that increase the risk of open surgery are poor candidates for a minimally invasive procedure. Those with significantly reduced forced expiratory volume may not tolerate the procedure and have an increased risk of requiring conversion to an open procedure.
Candidates for robotic hybrid revascularization must be able to undergo off-pump surgery with single-lung ventilation. Therefore, patients with severely impaired lung function and those with cardiogenic shock or hemodynamic instability are not appropriate candidates. Additionally, obesity, chest deformities, pleural adhesions and reoperation are generally contraindications, due to the technical difficulties they create.
Advertisement
The LAD artery must be accessible and not embedded in the myocardium. The patient must have a patent LIMA and no dialysis catheter or fistula in the left arm.
Hybrid revascularization is not appropriate for the patient who would benefit from all-arterial grafting, such as a 49-year-old male diabetic with a 90 percent lesion in the circumflex and LAD artery and 100 percent occlusion in the right coronary artery. Such a patient could benefit from bilateral internal mammary artery grafts and a radial graft, and it would be a disservice to perform PCI, which does not outperform arterial grafts.
To be eligible for robotic hybrid revascularization, the patient must be a candidate for both PCI and minimally invasive CABG. Ideally, this is a patient with multivessel disease, a complex LAD lesion and relatively simple non-LAD lesions that are amenable to PCI.
For instance, an active 70-year-old with LAD occlusion and right coronary artery stenosis (Figure) would be a suitable candidate. In such a case, we could perform a minimally invasive LIMA-to-LAD graft placement and stent the right coronary artery, producing revascularization likely to be equivalent in quality to open CABG.
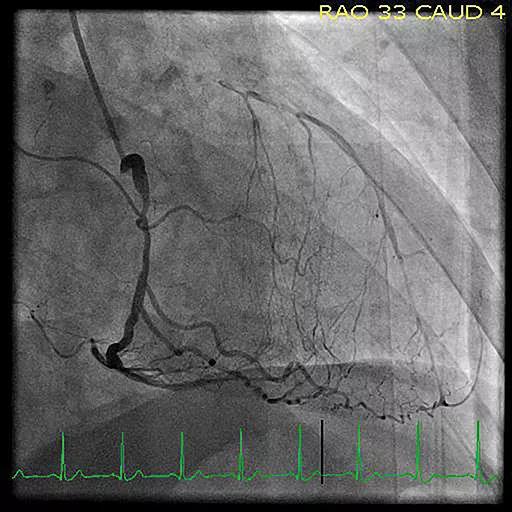
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/9338f1d7-b234-4978-9273-5bf7319b6c3e/RoboticHybrid-figure_jpg)
Figure. Catheterization image showing a totally occluded left anterior descending artery with right coronary artery stenosis, a combination that may prompt consideration of robotic hybrid revascularization.
Due to the complexity of the procedure, robotic hybrid revascularization may remain in the domain of a handful of medical centers where surgeons have mastered less-invasive CABG and have a late-generation da Vinci® robot in a cardiac surgery suite.
Advertisement
Nevertheless, as skills in robotic surgery improve and surgeons continue to refine minimally invasive CABG, we can expect to push the boundaries of the procedure to include patients with broader indications.
Dr. Mick is a staff surgeon in the Department of Thoracic and Cardiovascular Surgery whose specialty interests include robotically assisted procedures.
Advertisement
Advertisement

A sampling of outcome and volume data from our Heart & Vascular Institute

Concomitant AF ablation and LAA occlusion strongly endorsed during elective heart surgery

Large retrospective study supports its addition to BAV repair toolbox at expert centers

Young age, solid tumor, high uptake on PET and KRAS mutation signal risk, suggest need for lobectomy

Surprise findings argue for caution about testosterone use in men at risk for fracture

Residual AR related to severe preoperative AR increases risk of progression, need for reoperation

Findings support emphasis on markers of frailty related to, but not dependent on, age

Provides option for patients previously deemed anatomically unsuitable