Locations:

Emerging data offer reassurance of uncompromised efficacy

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/3a7a47e6-c284-4ad0-840d-bb73bd4006b8/690x380-Reduced-Radiation_jpg)
690×380-Reduced-Radiation
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
As fewer than 9 percent of pediatric cardiologists specialize in electrophysiology, research is essential to advancing knowledge in this subspecialty discipline. Cleveland Clinic Children’s Center for Pediatric and Congenital Heart Disease has a range of electrophysiology-related research projects underway.
One of them, profiled here, has yielded results with the potential to impact treatment of children with tachyarrhythmias by providing reassurance that radiation exposure can be curbed or eliminated during catheter ablation procedures without compromising efficacy.
The risks of radiation exposure are dose-dependent and cumulative over time, which makes reduction of radiation exposure in pediatric patients highly desirable. Radiation exposure can be decreased during catheter ablation with a relatively new technique using a 3-D electroanatomical navigation system. Major cardiac structures are mapped and used as reference points for tracking the location of the ablation catheter with magnets (Figure).
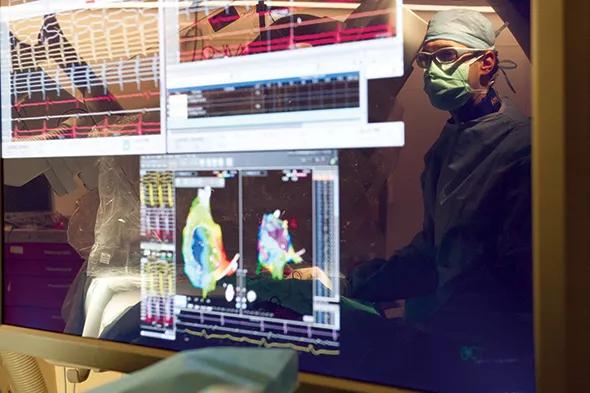
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/a6af0d76-5ed3-46b3-87bf-a5712d963ce1/590-Inset-Reduced-Radiation_jpg)
Figure. A snapshot of our “interface” of imaging using the 3-D electroanatomical navigation system. Intracardiac electrical tracings are shown during an atrial arrhythmia, along with the 3-D anatomical image of the right atrium (a large version of which is shown at the top of this post). These tools are used simultaneously and provide an excellent map for use in targeting ablation.
The system allows right heart ablation to be performed without fluoroscopy. When an arrhythmia is generated on the left side, fluoroscopy and intracardiac echocardiography are used to perform the transseptal puncture. However, ablation can be performed without fluoroscopy.
Advertisement
Because 3-D electroanatomical systems are relatively new, our understanding of their efficacy relative to that of conventional catheter ablation is still evolving. To fill gaps in that understanding, we reviewed the charts of 20 pediatric patients (mean age, 14.1 years) who underwent 3-D electroanatomical mapping for catheter ablations in the treatment of supraventricular tachyarrhythmias at Cleveland Clinic Children’s from October 2012 to May 2013.
All procedures were done by a single operator. Safety, efficacy and outcomes were compared with those of 20 age-matched control patients who underwent the same procedures by the same operator using conventional fluoroscopic guidance.
Although mean procedure time did not differ significantly between the two groups, mean fluoroscopy time was significantly lower with the 3-D mapping system (5.1 min) than with conventional fluoroscopic guidance (35.44 min) (P < .001). The average radiation dose was also significantly lower with 3-D mapping (7 mGy vs. 137.4 mGy; P < .0001). Twelve patients in the 3-D mapping group (60 percent) required no fluoroscopy use.
Acute procedural success was achieved in 18 of 20 patients in each group. Recurrence of the tachyarrhythmia was seen in only one patient in each group at follow-up.
We are currently adding more patients to this data set and will soon be publishing our full results.
When we began this study in 2012, only about 1 in 50 electrophysiologists was using the 3-D mapping system to minimize fluoroscopy. Today, that number may be closer to 1 in 15.
Advertisement
Because the system’s manufacturer does not currently offer courses on using the system, I am training electrophysiologists in its use here at Cleveland Clinic Children’s. Our adult electrophysiology fellows frequently adopt this technique and take it to their new practice settings after they complete their training. I believe that the sooner this new system can be adopted, the more quickly we can reduce radiation exposure in our patients, young or old.
Dr. Aziz is a pediatric electrophysiologist in the Department of Pediatric Cardiology in the Center for Pediatric and Congenital Heart Disease.
Advertisement
Advertisement

A sampling of outcome and volume data from our Heart & Vascular Institute

Concomitant AF ablation and LAA occlusion strongly endorsed during elective heart surgery

Large retrospective study supports its addition to BAV repair toolbox at expert centers

Young age, solid tumor, high uptake on PET and KRAS mutation signal risk, suggest need for lobectomy

Surprise findings argue for caution about testosterone use in men at risk for fracture

Residual AR related to severe preoperative AR increases risk of progression, need for reoperation

Findings support emphasis on markers of frailty related to, but not dependent on, age

Provides option for patients previously deemed anatomically unsuitable