Locations:

Favorable rates may stem from focus on outcomes monitoring

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/086aa1aa-2646-4941-abcf-655578daa85a/17-NEU-4300-Russman-Stroke-Outcomes-650x450_jpg)
17-NEU-4300-Russman-Stroke-Outcomes-650×450
After decades of decline, U.S. death rates from stroke have plateaued and even worsened in recent years, driven especially by trends in some areas of the country and among certain ethnic groups.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“Concerning national trends in recent years have highlighted the need for continued surveillance of stroke outcomes,” says Andrew Russman, DO, Medical Director of Cleveland Clinic’s Comprehensive Stroke Center.
Such surveillance has been the norm at Cleveland Clinic for years, and the latest outcomes findings reveal an encouraging bucking of these national trends. “Our data show that we are holding steady or doing better over time,” says Dr. Russman.
He’s referring to the bar graphs below showing annual in-hospital mortality from ischemic stroke (first graph) and intracerebral hemorrhage (second graph) at Cleveland Clinic over the years 2012 through 2016.
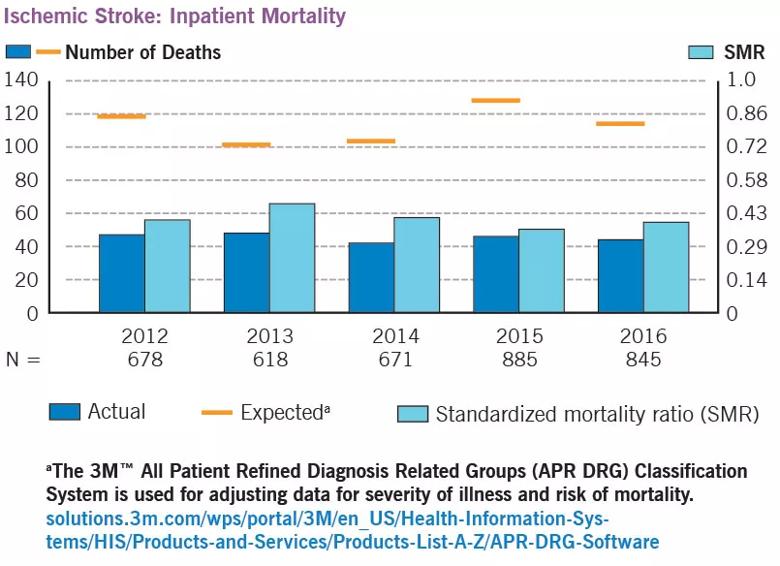
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/062e3eb0-1fe2-4eae-bee8-45266bda4634/17-NEU-4300-Russman-Stroke-Outcomes-inset1_jpg)
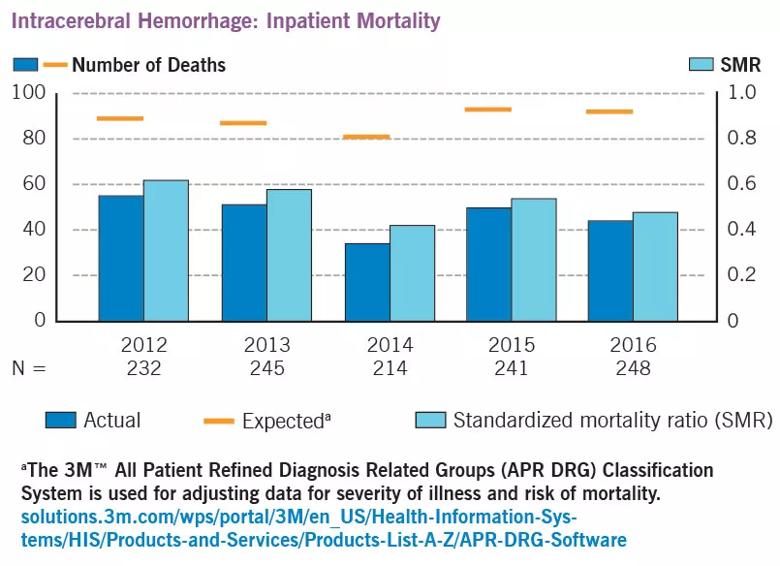
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/8863d3e5-2ac5-4b32-a2f5-dfdba8be83b2/17-NEU-4300-Russman-Stroke-Outcomes-inset2_jpg)
The graphs plot actual mortality at Cleveland Clinic against two benchmarks. The first is expected mortality, which is derived from the APR DRG system (see graph footnotes) and accounts for illness severity calculated from discharge billing codes and based on primary and secondary diagnoses, age and pre-existing conditions. The second benchmark is the standardized mortality ratio (SMR), which is the observed number of deaths divided by the number expected based on age- and sex-specific death rates in a standard population of stroke patients.
In every year, actual inpatient mortality for both stroke types was substantially lower than the expected rate — and in many cases approximately half the expected rate. Likewise, in every year the SMR was considerably less than 1.0 (see right vertical axis on each graph), indicating fewer deaths than expected.
Advertisement
Data on hospital length of stay were also collected for both stroke types, as detailed in the graphs below. In general, trends have been toward shorter stays over the past few years and mean stays have been shorter than expected based on APR DRG classifications.
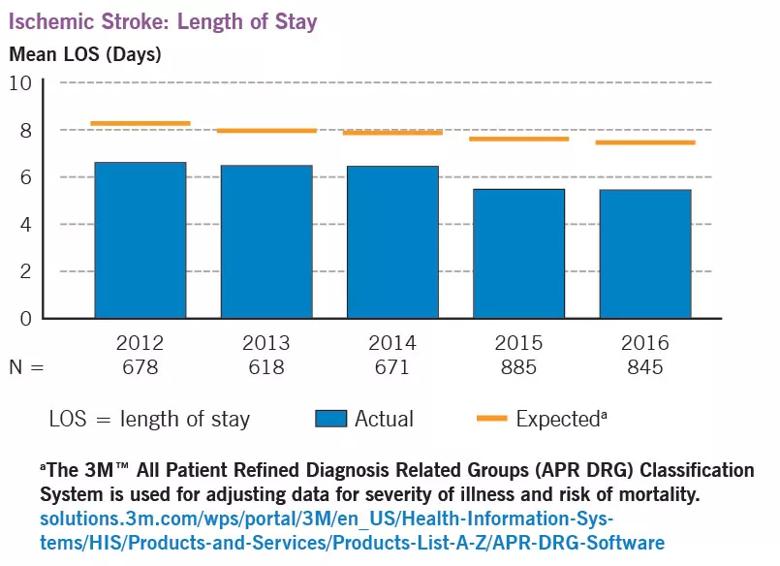
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/1218b50d-7fec-4025-9758-b316067b95ac/17-NEU-4300-Russman-Stroke-Outcomes-inset3_jpg)
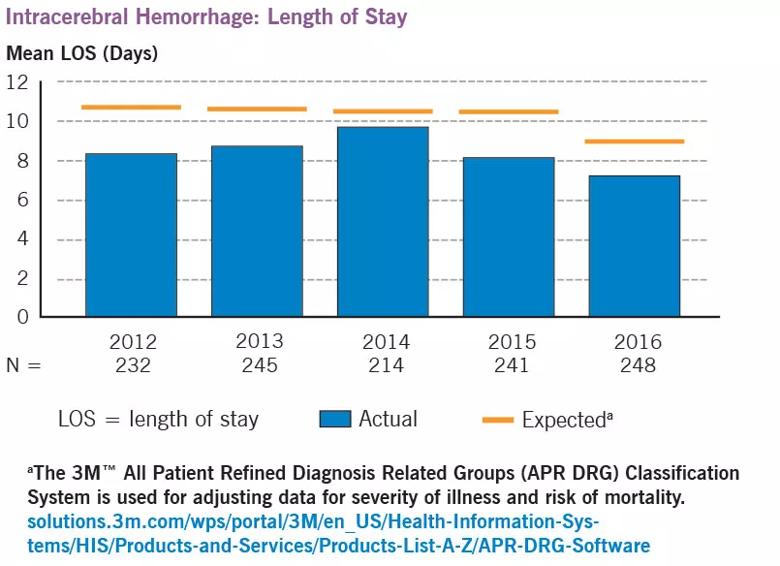
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/93ff610e-d84e-4c23-b52d-5b0f7a92788a/17-NEU-4300-Russman-Stroke-Outcomes-inset4_jpg)
Dr. Russman attributes the worsening national trends in stroke mortality to increasing obesity and the difficulty of controlling the associated risk factors for stroke, such as diabetes and hypertension. He says it’s uncertain why Cleveland Clinic’s stroke mortality rates have bucked these trends, but one contributing factor may be a highly collaborative approach. “We have an exemplary program for stroke care that brings together stroke neurologists, endovascular specialists, vascular neurosurgeons and neurointensivists in a single area to collaboratively manage patients as efficiently and effectively as possible,” he notes.
Another potential contributor is an openness to innovative approaches, as exemplified by Cleveland Clinic’s telemedicine-enabled mobile stroke treatment unit, the first of its kind in the country. This “emergency room on wheels” is summoned as an alternative to a standard ambulance when a 911 call is placed for someone experiencing stroke symptoms. The mobile unit contains blood testing capabilities, a CT scanner to assist in diagnosis and a telemedicine hookup to enable remote consultation with a stroke neurologist so that brain-saving measures can be started while the patient is en route to the hospital.
Advertisement
A final likely contributor is an abiding commitment to data-based continuous improvement. “We continually monitor our data and develop initiatives for process improvement,” Dr. Russman observes. “Detailed routine data collection like this can provide important insights for improving stroke care both at an institutional level and nationwide.”
These data and more are included in Cleveland Clinic’s comprehensive 2016 Neurological Institute Outcomes Book.
Advertisement
Advertisement

New study advances understanding of patient-defined goals

Testing options and therapies are expanding for this poorly understood sleep disorder

Real-world claims data and tissue culture studies set the stage for randomized clinical testing

Digital subtraction angiography remains central to assessment of ‘benign’ PMSAH

Cleveland Clinic neuromuscular specialist shares insights on AI in his field and beyond

Findings challenge dogma that microglia are exclusively destructive regardless of location in brain

Neurology is especially well positioned for opportunities to enhance clinical care and medical training

New review distills insights from studies over the past decade