Locations:

Two cases sketch out key decision-making factors

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/eece4b53-880f-4dff-bad9-c38aaa081c9a/HLBM-650-x-435_jpg)
HLBM 650 x 435
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Case 1. An 80-year-old man came to Cleveland Clinic for coronary artery bypass graft surgery (CABG) after being turned down for surgery at another institution. He had a history of prior stroke and a long smoking history. He presented with disease in his right coronary artery and left anterior descending and circumflex arteries, 85 percent stenosis of his right carotid artery, aortic calcifications and chronic obstructive pulmonary disease.
Case 2. A 52-year-old man was referred for surgical treatment of severe multivessel disease. He was a longtime diabetic who was otherwise in good health, physically active and employed.
Which of these patients would be best treated with on-pump CABG, and which with off-pump CABG?
CABG has been shown to significantly improve symptoms, quality of life and survival in patients with multivessel disease. However, the surgery is associated with a risk of stroke, myocardial infarction (MI), respiratory injury, renal injury and perioperative mortality. Techniques such as cardiopulmonary bypass, cardioplegia, aortic cannulation and cross-clamping are thought to be associated with these morbidities. By eliminating these factors, off-pump CABG may improve outcomes in selected patients.
But precisely who are those selected patients? In 2013, I participated in a consensus conference sponsored by the International Society for Minimally Invasive Cardiothoracic Surgery (ISMICS) that helps answer this question. Our goal was to determine whether off-pump CABG is superior to conventional on-pump CABG with respect to both clinical and resource-related outcomes, as well as to determine whether any such effects differed across prespecified risk groups and settings.
Advertisement
Our process included conducting a meta-analysis of clinical trials that served as the basis for consensus statements recently published in the ISMICS journal Innovations (2015;10:219-229) delineating the relative strengths and weaknesses of off-pump versus on-pump CABG — and clarifying who stands to benefit from each approach.
Our group reviewed all randomized controlled trials comparing on- and off-pump CABG published through April 2013 and selected 102 trials that met inclusion criteria for the meta-analysis. Of these trials, 15 enrolled 9,551 high-risk patients, and 87 enrolled 9,550 low-risk patients.
Primary end points of our analysis were all-cause mortality at 30 days and at more than one year. Secondary considerations were all-encompassing and included postoperative stroke, cognitive dysfunction, acute MI, recurrent angina, coronary reintervention, need for inotropes, need for intra-aortic balloon pump, atrial fibrillation, renal failure, mediastinitis/sternal wound infection, respiratory infection, need for blood transfusion, re-exploration for bleeding, mechanical ventilation time, ICU length of stay (LOS), hospital LOS, hospital costs and quality of life.
No significant differences were seen between on- and off-pump CABG in multiple parameters (see table). The meta-analysis showed that off-pump CABG offers benefits in patients at risk for complications from cardiopulmonary bypass, as it was associated with reduced risk of stroke, renal dysfunction/failure, blood transfusion, respiratory failure, atrial fibrillation and wound infection as well as reductions in ventilation time and both ICU and hospital LOS.
Advertisement
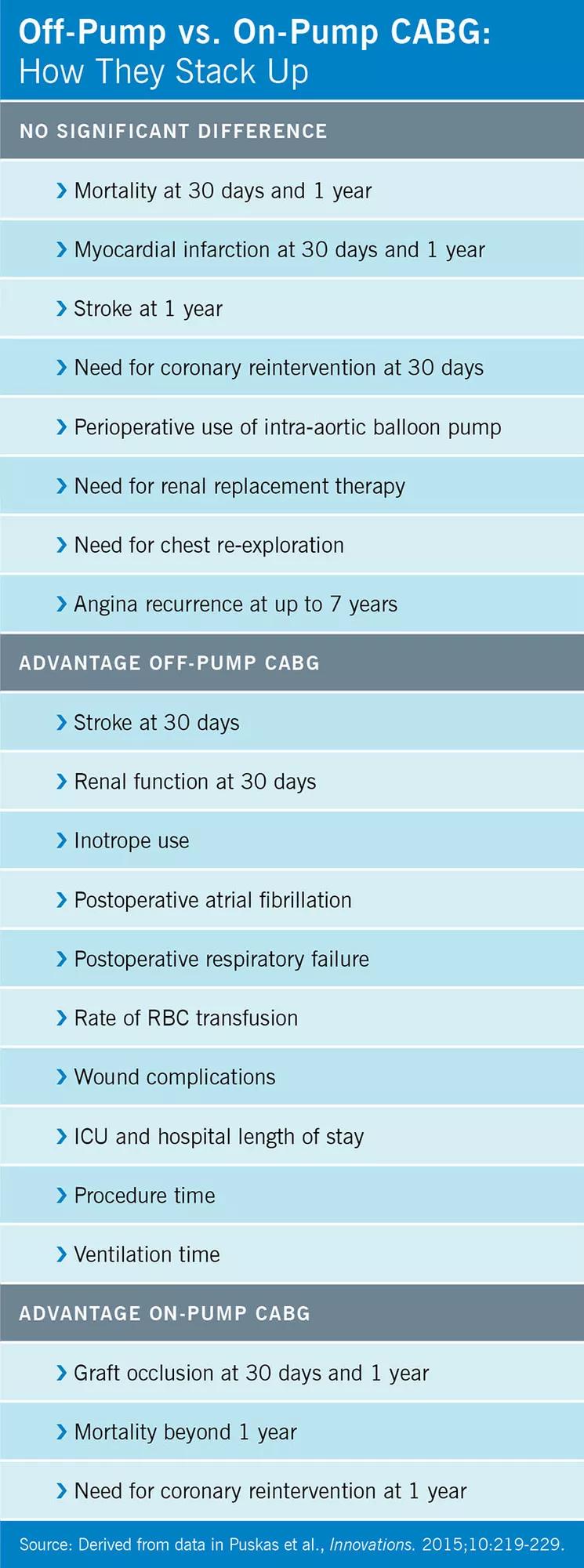
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/c7aba2fe-edd4-4683-bc69-f03761bdd1e6/16-HRT-293-OnVsOffPumpCABG-CQD-chart_jpg)
The main weakness of off-pump CABG was — and continues to be — the risk of less-successful revascularization, as it was associated with a reduced number of grafts and diminished graft patency. Also, compared with on-pump procedures, off-pump CABG improved short-term outcomes but was associated with increased risk of coronary reintervention at one year and perhaps with increased mortality beyond one year.
Let’s apply these insights to the first of our two cases from the beginning — the 80-year-old gentleman who needed only two grafts. Because long-term patency was less a concern for this patient than were short-term complications, he was an excellent candidate for off-pump CABG.
When a patient has complex disease, needs multiple grafts and is at low risk from cardiopulmonary bypass, conventional on-pump CABG remains the better approach for revascularization.
In light of that, consider our 52-year-old patient from the beginning: He had good kidney function, good lungs and no aortic atherosclerosis, so his risk of pump-related complications was low. In order to confer optimal long-term revascularization, for this patient we ended up choosing on-pump CABG using all arterial grafts.
As cardiothoracic surgeons, we must be able to perform both on- and off-pump CABG procedures. Any practice that uses either approach exclusively is fitting the patient to the operation rather than fitting the operation to the patient.
At Cleveland Clinic, we review the patient’s information and recommend whether the operation should be done on or off pump. In a small percentage of cases, we change course during surgery — for example, the discovery of extensive aortic atherosclerosis in a patient undergoing on-pump CABG may require conversion to off-pump surgery. But with today’s excellent imaging techniques, that seldom happens.
Advertisement
Dr. Sabik is Chair of Thoracic and Cardiovascular Surgery at Cleveland Clinic.
Advertisement
Advertisement

A sampling of outcome and volume data from our Heart & Vascular Institute

Concomitant AF ablation and LAA occlusion strongly endorsed during elective heart surgery

Large retrospective study supports its addition to BAV repair toolbox at expert centers

Young age, solid tumor, high uptake on PET and KRAS mutation signal risk, suggest need for lobectomy

Surprise findings argue for caution about testosterone use in men at risk for fracture

Residual AR related to severe preoperative AR increases risk of progression, need for reoperation

Findings support emphasis on markers of frailty related to, but not dependent on, age

Provides option for patients previously deemed anatomically unsuitable