Locations:

Novel outpatient model promises to refine and rationalize AED therapy

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/cf95aefa-ab98-4f80-969b-01e69092ab91/18-NEU-5933-cEEG-650x450_jpg)
18-NEU-5933-cEEG-650×450
A clinic dedicated to systematic follow-up of patients with new onset of seizures during hospitalization enables critical monitoring of epilepsy development and assessment of medication needs. So concluded Cleveland Clinic epileptologist Vineet Punia, MD, MS, in two poster presentations at the American Epilepsy Society’s 2018 annual meeting in early December.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Dr. Punia detailed Cleveland Clinic’s first year of experience with the Post-Acute Symptomatic Seizure (PASS) clinic, a novel outpatient care model for patients newly identified with seizures during hospitalization. Half of the patients seen at the epileptologist-staffed clinic needed their antiepileptic drugs (AEDs) either reduced, increased or switched.
“With increasing use of continuous EEG monitoring during hospitalization, more and more patients with no previous diagnosis of epilepsy are being discharged on antiepileptic drugs,” explains Dr. Punia. “Such patients need monitoring by an epileptologist to check if their medications are appropriate over the longer term, but they are often lost to follow-up.”
In May 2017, Cleveland Clinic instituted a “best practice advisory” (see example below) to notify discharge providers when a patient meets the following criteria for a follow-up appointment with the PASS clinic: (1) undergoing continuous EEG monitoring during admission, (2) having no prior history of epilepsy and (3) being discharged on an AED. Two orders automatically pop up in Cleveland Clinic’s electronic medical record system for such patients at the time of hospital discharge:
The orders are either approved or declined by the healthcare provider, then automatically routed to the PASS clinic scheduler to contact the patient.
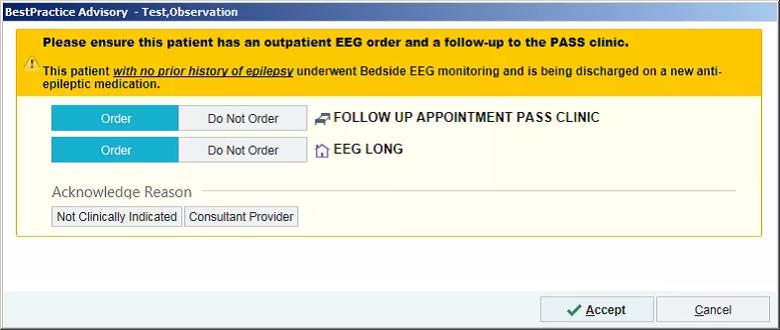
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/852165d7-b35f-46a4-8c71-552b3dfd79eb/18-NEU-5933-EMR-alert_Inset_png)
Dr. Punia reported on the first 12 months’ data from the PASS clinic following institution of the best practice advisory alerts. During that time, 184 patients (mean age, 60.6 years) were scheduled for a PASS clinic appointment at discharge. Of those, 50 died before their appointment, 50 cancelled and 35 were no-shows.
Advertisement
The remaining 49 patients were seen in the PASS clinic, and all but three were still taking an AED at the time of their visit, which took place 117 days after discharge, on average. As a result of the visit, medications were adjusted for those 46 patients as follows:
“Many of the PASS clinic patients had subclinical seizure activity during their hospitalization or seizures while they were comatose, so they had no idea why they were put on AEDs,” says Dr. Punia. “Educating these patients is important so that they are motivated to continue appropriate therapy and monitoring.”
He adds that nine of the 49 patients (18.4 percent) had more seizures in the interval between hospital discharge and their PASS clinic appointment, making the need for follow-up care with an epileptologist especially critical.
Dr. Punia notes that recently published studies underscore the importance of the PASS clinic model:
Dr. Punia is lead author of two studies from Cleveland Clinic Epilepsy Center (J Clin Neurophysiol. 2018;35:71-76 and Epilepsy Behav. 2015;49:250-254) that found that although only a minority of patients with lateralized periodic discharges and no history of epilepsy developed epilepsy over the next 10 to 30 months, most patients remained on AEDs at long-term follow-up.
Advertisement
“Most physicians in general practice are reluctant to manage AEDs and reduce or stop their use, especially in the vulnerable, high-risk patients who tend to have had continuous EEG monitoring,” he notes. “Indiscriminate long-term use of AEDs is a real concern.”
He explains that side effects of AEDs — such as lethargy and fatigue — are often similar to effects experienced during recovery from a stroke or other brain injury, which adds to the uncertainty surrounding AED use and makes it more critical that patients be taken off unnecessary neurological drugs.
Dr. Punia says he’s received a great deal of interest from neurologists and epileptologists at other centers in setting up services like the PASS clinic. Based on Cleveland Clinic’s experience, he advises the following:
“More clinics like the PASS clinic will enhance collaborative research and improve care,” concludes Dr. Punia. “I look forward to the emergence of a multi-institutional network for data sharing.”
Advertisement
Advertisement

New study advances understanding of patient-defined goals

Testing options and therapies are expanding for this poorly understood sleep disorder

Real-world claims data and tissue culture studies set the stage for randomized clinical testing

Digital subtraction angiography remains central to assessment of ‘benign’ PMSAH

Cleveland Clinic neuromuscular specialist shares insights on AI in his field and beyond

Findings challenge dogma that microglia are exclusively destructive regardless of location in brain

Neurology is especially well positioned for opportunities to enhance clinical care and medical training

New review distills insights from studies over the past decade