Locations:

Diagnosis is tricky but must be urgent to avert irreversible damage

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/87457acd-c798-46d2-8fba-b1f12291d36a/IE-690x380_jpg)
IE-690×380
Infective endocarditis (IE) affects 20,000 to 50,000 U.S. adults a year. Without prompt diagnosis and proper treatment, damage to the valve and myocardium may be irreversible and lead to complications such as heart failure, sepsis, stroke and renal failure.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
In IE, microorganisms adhere to areas of damaged endocardium and form vegetations. Infected tissue can split off emboli, which may occlude arteries in the brain and other organs, causing local infarcts, mycotic aneurysms and infection. Bacteria also produce toxins and enzymes that kill normal cells and disintegrate the tissue, damaging leaflets and preventing cusps from healing.
“The diagnosis and management of patients with IE requires a multidisciplinary, team-based approach involving clinicians with knowledge about the disease process and experience treating patients at each step,” says Steven Gordon, MD, Chairman of the Department of Infectious Disease and a member of Cleveland Clinic’s IE team.
The team — which also comprises clinical and interventional cardiologists, cardiothoracic surgeons, pathologists, microbiologists, neurologists and psychiatrists — has accrued one of the largest single-center experience bases with IE in the world.
Challenges start with making a diagnosis early, before damage advances.
Patients commonly present with fever and may complain of muscle and joint aches and poor appetite, making IE an easy diagnosis to overlook. Risk factors for IE include previous heart disease, interventional procedures, implanted prosthetic devices or dental work.
“You have to have a high level of suspicion and avoid jumping to the conclusion that the patient has influenza with pneumonia and immediately prescribe antibiotics,” says Gösta Pettersson, MD, PhD, Vice Chairman of the Department of Thoracic and Cardiovascular Surgery.
Advertisement
Such suspicion is particularly important if the patient has a prosthetic valve or other cardiac device, he adds. “Any patient with a history of valve surgery who becomes febrile and does not improve quickly should be referred to a center with experience diagnosing IE.”
Even when echocardiography shows no sign of infection, infected tissue may be lurking. Three separate blood cultures from different venipuncture sites should be obtained at least one hour apart to confirm the diagnosis and identify the pathogen, Dr. Pettersson notes.
“The pathology is important, because it describes the stage of disease as it relates to the damage caused by the infection and predicts which problems will develop,” he explains.
In acute cases, antibiotic treatment should be started within two hours, during which time the blood cultures are being obtained. “To prevent valve damage, antibiotics have to be started before destruction begins,” Dr. Pettersson says.
Waiting for antibiotics to clear the infection before taking further action is a classic mistake, say the IE experts. The antibiotic may not be effective, and the disease will worsen. Prompt removal of infected tissue may be required.
“Not every patient needs surgery, but every case should be evaluated with an experienced cardiac surgeon,” says Dr. Gordon.
Knowing when to operate before damage occurs requires experience. “The surgeon is often involved too late, when valve destruction is advanced,” says Syed Hussain, MD, a cardiothoracic surgeon on the IE team.
Advertisement
If infection is not entirely debrided, the patient will have an increased risk of recurrent infection and death. Risk is further increased in patients with a prosthetic valve. Unfortunately, some physicians are hesitant to send these patients for a second surgery.
“By the time we see them, they are often extremely sick and need a more complex operation,” says Dr. Hussain.
Early referral may save the valve, avoid an operation and lower the risk of death. In experienced centers, surgery in patients with active IE is today associated with much lower mortality than before. In a review of 1,195 consecutive patients who underwent surgery for IE at Cleveland Clinic from 2002 through 2010, 30-day survival was 92 percent, with similar survival for patients with prosthetic and natural valve infections (Figure 1).
For patients with destruction and invasive IE, outcomes are better if the IE affects the aortic valve rather than the mitral valve (Figure 2). Reasons include the typically poor condition of patients with mitral valve IE, the mitral valve anatomy and less-than-optimal mitral valve prostheses.
“If you postpone surgery on the presumption that operating on a patient with active infection is too risky and technically demanding, you may expose the patient to risk of further cardiac tissue destruction and potential development of heart failure, heart block and repeat embolic events,” says Dr. Pettersson. “It also increases the possibility that the patient may subsequently be ineligible for surgery due to complications of the disease or its treatment.”
Advertisement
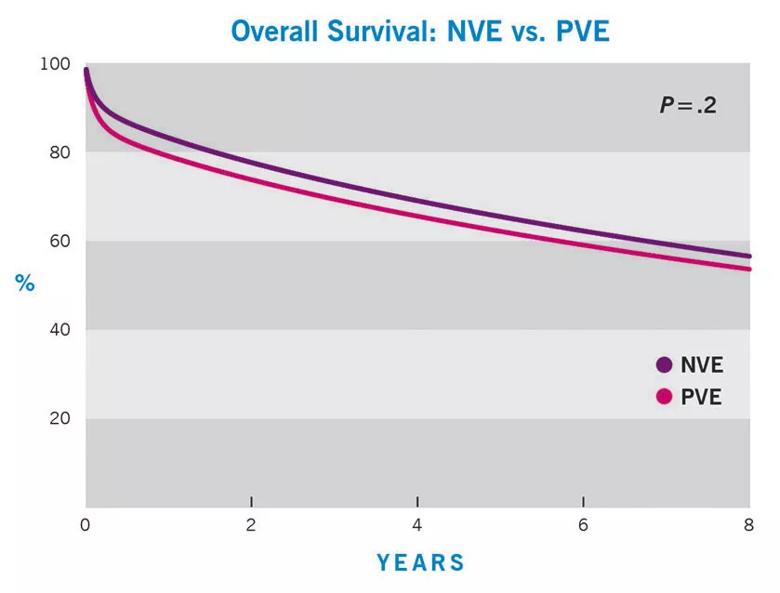
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/883857a2-ffcf-456f-86be-cfcf5631da08/Endocarditis_graph_1_jpg)
Figure 1. Survival among 1,195 patients who had surgery for IE at Cleveland Clinic from 2002 through 2010 was comparable regardless of whether patients had prosthetic (PVE) or natural (NVE) valve endocarditis. Overall survival in the combined groups was 92 percent at 30 days, 81 percent at one year, 72 percent at three years and 60 percent at seven years.
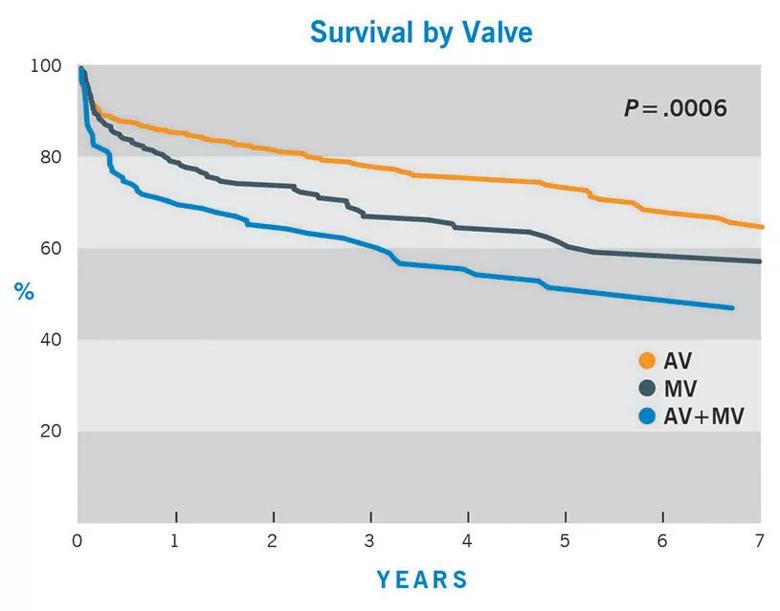
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/99417db3-7a08-463c-bfeb-4b09f892b510/Endocarditis_graph_2_jpg)
Figure 2. Among the same cohort of patients as in Figure 1, survival varied significantly by whether IE involved the aortic valve (AV), the mitral valve (MV) or both.
Because understanding the pathophysiology of IE is critical to understanding its natural progression and choosing the optimal operation for the best outcome,.Dr. Pettersson and colleagues have condensed this information into nine pearls of wisdom in a liberally illustrated atlas of IE disease progression published in the April 2014 Journal of Thoracic and Cardiovascular Surgery.
“The atlas presents major concepts that collectively describe the main features and basic facts about endocarditis every surgeon needs to know,” Dr. Pettersson says.
The concepts are:
Advertisement
Contact Dr. Pettersson at petterg@ccf.org, Dr. Hussain at hussais2@ccf.org and Dr. Gordon at gordons@ccf.org.
Advertisement

A sampling of outcome and volume data from our Heart & Vascular Institute

Concomitant AF ablation and LAA occlusion strongly endorsed during elective heart surgery

Large retrospective study supports its addition to BAV repair toolbox at expert centers

Young age, solid tumor, high uptake on PET and KRAS mutation signal risk, suggest need for lobectomy

Surprise findings argue for caution about testosterone use in men at risk for fracture

Residual AR related to severe preoperative AR increases risk of progression, need for reoperation

Findings support emphasis on markers of frailty related to, but not dependent on, age

Provides option for patients previously deemed anatomically unsuitable