Locations:

7 tips for better, multidisciplinary obesity care

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/dc2942a5-56aa-4575-8f21-3e7c0fb8bf71/19-END-4008-Treat-Obesity-CQD_jpg)
19-END-4008-Treat-Obesity-CQD
Many patients with severe obesity (class 3, body mass index [BMI] 40 kg/m2) receive suboptimal care, a recent article in Mayo Clinic Proceedings suggests. With a primary focus on managing chronic conditions, clinicians may fail to treat their underlying cause.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Associated with heart disease, cancer and diabetes, severe obesity significantly reduces life expectancy. In the decade between 2000 and 2010, the prevalence of severe obesity increased by 70%. Although medical treatments for severe obesity exist—such as bariatric surgery and pharmacotherapy—even patients who receive regular medical care for chronic conditions are unable to lose weight.
“Obesity is mainly responsible for the onset of the majority of chronic conditions that we treat daily in our clinics, but it is also a chronic disease in its own right,” says Bartolome Burguera, MD, PhD, Chairman of Cleveland Clinic’s Endocrinology & Metabolism Institute and lead author on the paper. “We need to work together with patients to change the old medical paradigm of treating the chronic conditions likely caused by excess weight, but not appropriately addressing obesity.”
In this most recent paper, Dr. Burguera and his colleagues suggest several steps that physicians can take to help their patients with severe obesity. These include:
Advertisement
“I’ve worked at medical institutions on both sides of the Atlantic Ocean, and I’ve learned that patients with obesity are discriminated against, both explicitly and implicitly, regardless of where they live,” Dr. Burguera explains. “These patients are often treated with bias by their colleagues and, in many circumstances, by their physicians. I listen to patients with empathy and respect. I need to understand their concerns in order to work with them to develop therapeutic plans.”
Under Dr. Burguera’s leadership, Cleveland Clinic has developed an interdisciplinary approach that includes working with the Employee Health Plan, and is centered on nutrition, physical activity, appetite control and optimization of sleeping habits, as well as psychological support focused on stress reduction and the treatment of anxiety and depression.
“In the next several years, we will continue to find innovative ways to treat patients with a focus on compassion and convenience. We want to create relaxed, supportive, personalized environments for the exchange of information,” Dr. Burguera says.
Advertisement
Advertisement

Radiofrequency ablation significantly reduces symptom severity, shrinks nodules

Maternal-fetal medicine specialists, endocrinologists and educators team up

Giving young patients a hand as they take charge of their own health

Case illustrates how easily condition can mimic preeclampsia
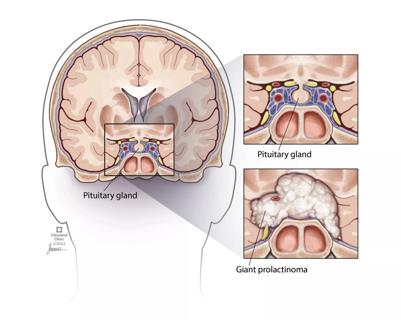
Analysis examines surgical resection of rare pituitary tumors
Screening and medication key to better outcomes

Spinal cord stimulation can help those who are optimized for success
Incidence, outcomes and management