Locations:

Backdrop to a novel trans-conal unroofing approach to a rare defect
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Success in surgery for congenital heart disease is inseparable from two things: the way an institution’s program is organized, and the program’s readiness to innovate at any turn.
At Cleveland Clinic, we optimize congenital heart surgery outcomes by starting before the infant with a congenital defect is born and carefully detailing every step in advance to expedite the newborn’s first surgery and subsequent procedures.
Our experience also allows us to innovate. At the upcoming Society of Thoracic Surgeons annual meeting in San Diego, we will be presenting a novel approach to a rare congenital heart defect: anomalous aortic origin of left main coronary artery (LMCA) arising from right coronary sinus with posterior extension of the right ventricular outflow tract.
Rather than performing a bypass, we have used trans-conal unroofing to produce successful outcomes in five patients. All were adults, but our experience with surgical approaches to congenital malformations directly informed our development of the new surgical approach.
In all five surgeries, we used a trans-conal approach for extensive unroofing of the intraseptal LMCA, followed by patch augmentation of the posterior wall of the right ventricular outflow tract (Figure). The trans-conal approach gives direct exposure of the full length of the LMCA for effective mobilization of the proximal kinked segment and full muscular unroofing of the body of the artery. Posterior extension of the right ventricular outflow tract helps avoid arterial compression during exercise.
Advertisement
All five patients — who ranged in age from 35 to 60 years — have undergone their operations within the past year, and all are doing well. All had ischemia preoperatively, but none do now. We continue to follow them.
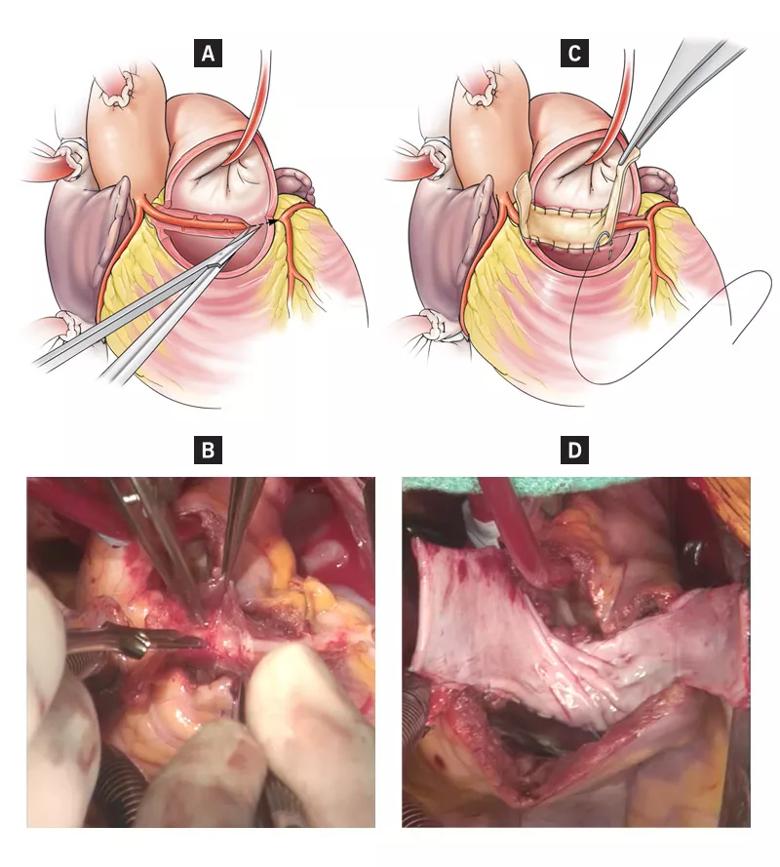
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/5c301682-6e24-4e38-9acf-ced962206316/18-HRT-5874-Najm-CQD-Inset_jpg)
Figure. Key steps in our novel trans-conal unroofing procedure. (A) Schematic illustration of the division of the right ventricular outflow tract (RVOT). (B) Photo of the unroofed left main coronary artery behind the RVOT. (C and D) Illustration and surgical photo of the autologous pericardial patch extension of the RVOT.
New approaches such as this have contributed to our improved outcomes. In 2018, Cleveland Clinic’s 30-day mortality rate was zero across more than 400 congenital heart disease surgeries, with one late mortality. This compares well with the typical 3 percent rate across the nation (according to the Society of Thoracic Surgeons Congenital Heart Surgery Database). This means that outcomes are more than 10 times better than the national average and that an extra 12 patients left Cleveland Clinic’s congenital heart disease program alive and well than would have been the case had they been operated on at another center.
We attribute this success not to fancy machines or devices but to the ability to diagnose early, do proper surgery and care for our patients appropriately after surgery. That’s why patient survival is higher than at other centers.
For the best surgical outcomes in congenital heart disease, it’s important to make the diagnosis during pregnancy whenever possible, usually by fetal echocardiography between 18 and 25 weeks’ gestation. Our heart surgery team makes the diagnosis and counsels the parents about the nature of the lesion, the anticipated surgery and its timing, and the expected outcome.
Advertisement
Sometimes surgery is necessary within hours of birth. An example would be an in utero diagnosis — confirmed via fetal echo — of univentricular or biventricular obstructed total anomalous pulmonary venous drainage. Once the obstruction occurs, any delay in management compounds the damage.
We handle such cases in Cleveland Clinic’s Special Delivery Unit (SDU). A mother comes in for a planned cesarean section, which is performed at 7:30 a.m. Within hours, the baby is in the OR receiving open-heart surgery. We’re able to do this because the SDU is across the corridor from the catheterization lab and right next to the OR. There is no wasted time or transport.
About 70 percent of infants with congenital heart disease will have simple defects that can be repaired in one procedure, although they all require lifelong monitoring. Some patients, such as those with tetralogy of Fallot, will require a pulmonary valve implant at some point in their adult lives, sometimes decades later.
But infants born with univentricular hearts will require a series of staged operations. Typically this involves a Norwood procedure, a shunt or band at or near birth, a bidirectional Glenn anastomosis at age 4 to 6 months, and a Fontan procedure at age 2 to 4 years.
Patients will usually remain cyanotic until they receive the Fontan procedure, after which they should turn a healthy pink. At this point, those without comorbid developmental problems can lead relatively normal lives with just a single pumping chamber, although they must always avoid competitive sports.
Advertisement
Dr. Najm is Chair of Pediatric and Congenital Heart Surgery at Cleveland Clinic.
Advertisement
Advertisement

A sampling of outcome and volume data from our Heart & Vascular Institute

Concomitant AF ablation and LAA occlusion strongly endorsed during elective heart surgery

Large retrospective study supports its addition to BAV repair toolbox at expert centers

Young age, solid tumor, high uptake on PET and KRAS mutation signal risk, suggest need for lobectomy

Surprise findings argue for caution about testosterone use in men at risk for fracture

Residual AR related to severe preoperative AR increases risk of progression, need for reoperation

Findings support emphasis on markers of frailty related to, but not dependent on, age

Provides option for patients previously deemed anatomically unsuitable