Locations:

Need for activity limits can make return to play a tough call

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/69220c04-a313-4714-a4c8-aa2c644b351c/690x380-DeMicco_jpg)
690×380-DeMicco
By Russell DeMicco, DO
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Made up of the Greek roots for “vertebra,” “break” and “slipping,” spondylolysis refers to a defect in the pars interarticularis (the segment of the vertebral arch lying between the superior and inferior articular processes) and spondylolisthesis refers to a defect with slipping of one vertebra on another.
Both conditions are relatively common in children and adolescents. Spondylolysis may be present in 5 to 10 percent of a normal population and is the most common cause of spondylolisthesis. There is a higher incidence of spondylolysis in certain populations, including athletes— particularly gymnasts, divers, football linemen, tennis players, divers and rowers.
Symptoms of these conditions may include dull, aching low back pain that is worsened with athletic activities. Repetitive flexion/extension motion is thought to be a key factor in the development of spondylolysis and aggravation of painful symptoms.
Physical exam findings in patients with these conditions may include tight hamstrings, crouched or waddling gait, or even palpable step-off.
Although the history and physical exam findings may raise the level of suspicion, the diagnosis is confirmed with imaging.
Standing anteroposterior and lateral lumbar radiographs (Figure 1) help define any underlying alignment concerns that may be missed on studies while the patient is lying down. Spondylolysis can be appreciated on oblique lumbar radiographs. Advanced imaging studies (MRI, CT, and bone scan with SPECT) can provide greater detail and help determine the treatment course.
Advertisement
The Meyerding grading classification is used to describe the degree of slippage of the upper vertebra on the lower one:
The most common type of spondylolisthesis is the isthmic or spondylolytic spondylolisthesis, which can be divided into subtypes as follows:
The treatment of patients with spondylolysis or spondylolisthesis ranges from observation to restriction of activities/athletics, bracing and surgery. Simple medications (e.g., acetaminophen or NSAIDs such as ibuprofen or naproxen) and education are often the first steps in management.
Advanced imaging aids in determining the acuity of spondylolysis. Response to bracing is more predictable and favorable with acute process without evidence of bony sclerosis. The braces/spinal orthoses are used to maintain lumbar flexion to counteract extension forces through the pars.
Because activity restriction is a component of early management in many cases, return-to-play considerations can be difficult. Here is our general guidance formanagement of these conditions:
Advertisement
Thankfully, the number of patients undergoing surgery for these problems is low compared with the total identified. Imaging is useful in identifying problems and guiding management.
Surgical options include repair of the pars defect or segmental fusion across the disk. When surgery is needed, the surgical approach used and the path to return to play are typically decided among the spine physician, the patient and his/her family, and the patient’s athletic trainer or physical therapist. Return to play is determined on a case-by-case basis with input from all the above parties.
Healing of a spondylolysis is confirmed when resolution of edema can be seen on certain MRI sequences (STIR sequences are best; T2- and T1-weighted images also may show pathology).
Pain is typically the factor that limits return to play, so if we can control pain and allow healing, most patients will successfully return.
Dr. DeMicco is a medical spine specialist and Co-Director of the Spine Medicine Fellowship in the Center for Spine Health.
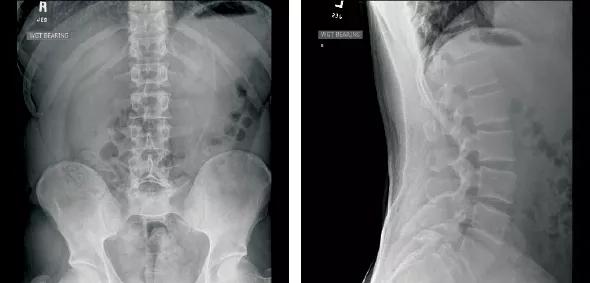
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/684cbd07-0178-4612-9345-7fd05e1d5596/590x-Inset-DeMicco_jpg)
Figure 1. Anteroposterior (left) and lateral (right) lumbar radiographs in a patient with defects of the pars interarticularis at L5 with spondylolisthesis of L5 on S1. The patient was treated successfully without surgery.
Advertisement
Advertisement

New study advances understanding of patient-defined goals

Testing options and therapies are expanding for this poorly understood sleep disorder

Real-world claims data and tissue culture studies set the stage for randomized clinical testing

Digital subtraction angiography remains central to assessment of ‘benign’ PMSAH

Cleveland Clinic neuromuscular specialist shares insights on AI in his field and beyond

Findings challenge dogma that microglia are exclusively destructive regardless of location in brain

Neurology is especially well positioned for opportunities to enhance clinical care and medical training

New review distills insights from studies over the past decade