Locations:

Avoiding complex reoperative abdominal surgery and ostomy
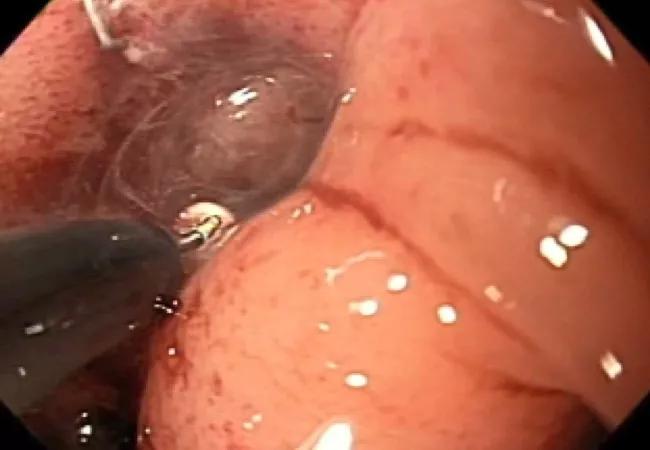
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/9141d63f-6ec9-43c5-b3cf-ee8ceb72fe7c/17-DDI-3753-Endoscopic-Sinusotomy-CQD_jpg)
17-DDI-3753-Endoscopic-Sinusotomy-CQD
By Bo Shen, MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
The Interventional Inflammatory Bowel Disease Unit at Cleveland Clinic’s Digestive Disease & Surgery Institute is a pioneer and world leader in the endoscopic management of IBD and colorectal surgery-associated complications.
For the past decade, we have developed a range of novel endoscopic techniques to manage strictures, fistula, anastomotic leak and abscess, including endoscopic stricturotomy, endoscopic sinusotomy, endoscopic septectomy, endoscopic fistulotomy, endoscopic incision and drainage, endoscopy-guide seton and drainage catheter placement.
A 65-year-old man was transferred to our hospital service from out of state for an acute presacral anastomotic leak with a large hematoma, resulting in severe rectal bleeding that required blood transfusion.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/087eb6ba-d760-4481-adde-26b487453a9a/long-sinus-tract_jpg)
The long sinus track from the anastomosis.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/3121b901-486b-4c63-90e9-598b40557548/treated-sinus-tract_jpg)
Treated sinus track, almost resolved.
The patient had undergone partial colectomy, colorectal anastomosis and ileostomy for advanced rectal cancer and radiation therapy. The bleeding failed to respond to therapy with endoscopic hemoclips and epinephrine injection.
The interventional endoscopist was able to successfully control the bleeding with an innovative instillation of hyperosmolar dextrose via endoscopy and enemas. After cessation of bleeding, the presacral hematoma was replaced by a 3.5 cm anastomotic sinus.
Subsequently, the presacral sinus was completely healed with two sessions of endoscopic sinusotomy with isolated knife tip (see main image above), which was pioneered at Cleveland Clinic. Each session of this outpatient endoscopic procedure took 15 minutes with the patient under conscious sedation. The recovery time for each procedure was 30 minutes.
Advertisement
The patient was ultimately able to have stoma closure and avoid a permanent ostomy.
Wu XR, Wong RC, Shen B. Endoscopic needle-knife therapy for ileal pouch sinus: a novel approach for the surgical adverse event (with video). Gastrointest Endosc. 2013;78:875-885.
Shen B. Exploring endoscopic therapy for the treatment of Crohn’s disease-related fistula and abscess. Gastrointest Endosc. 2017;85:1133-1143.
Advertisement
Advertisement

Strong patient communication can help clinicians choose the best treatment option

ctDNA should be incorporated into care to help stratify risk pre-operatively and for post-operative surveillance

The importance of raising awareness and taking steps to mitigate these occurrences

New research indicates feasibility and helps identify which patients could benefit

Treating a patient after a complicated hernia repair led to surgical complications and chronic pain

Standardized and collaborative care improves liver transplantations

Fewer incisions and more control for surgeons

Caregiver collaboration and patient education remain critical