Locations:

Indications span a vast array of common problems
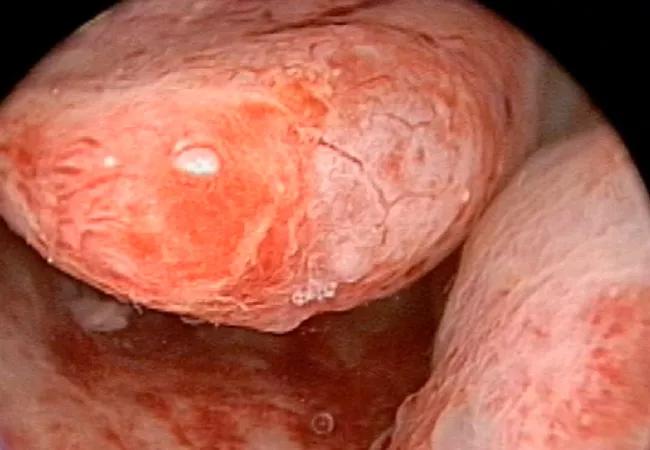
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/8414e05f-914e-45fa-8308-ac388e324734/Bradley-09_01_2017_cystic-varigated-submucosal-fibroid_650x450_jpBRADLEY_g_jpg)
Bradley 09.01.2017_cystic-varigated-submucosal-fibroid_650x450.jpBRADLEY_g
With an estimated 90 percent of hysterectomies performed for non-life-threatening indications, including uterine fibroids and uterine bleeding, Cleveland Clinic gynecologist Linda D. Bradley, MD, Director of the Fibroid and Menstrual Disorders Center and Director of Hysteroscopic Services, is an outlier.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
To effectively reduce the need for hysterectomies, Dr. Bradley champions the use of hysteroscopy for the evaluation of patients with abnormal menstrual periods, infertility, recurrent miscarriage, retained products of conception, endometrial polyps, intrauterine fibroids, abnormal bleeding and, in some cases, abnormal Pap results. Over time, she has convinced her colleagues in the Ob/Gyn & Women’s Health Institute to carry the hysteroscopy banner and is now urging others to do the same.
“Urologists use cystoscopes to investigate urinary tract bleeding with hematuria. Pulmonologists use bronchoscopes on patients who are coughing up blood. An orthopod will use an arthroscope to look inside a painful knee. Yet gynecologists have not fully embraced hysteroscopes like other specialties have for symptomatic problems,” says Dr. Bradley, who is also institute Vice Chair.
“My hysteroscope is my stethoscope!” she adds.
Hysteroscopy offers multiple benefits for physicians and patients alike.
“Hysteroscopy can be a comfortable, office-based, economically wise technique for taking a look that offers the best use of time and resources. It enables me to evaluate endometrial health and then plan the appropriate surgical procedure or make a referral,” she says.
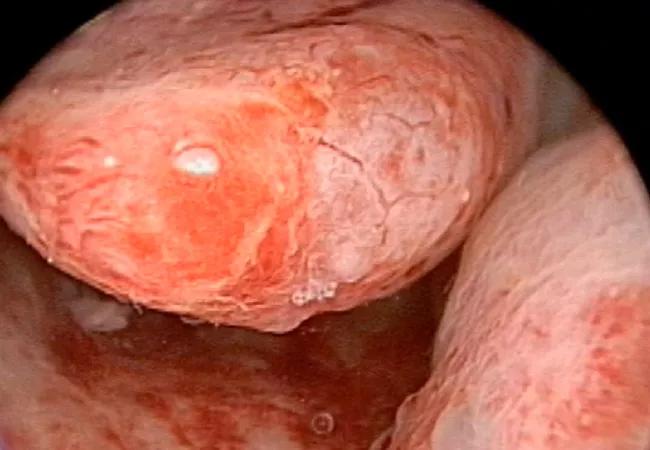
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/8414e05f-914e-45fa-8308-ac388e324734/Bradley-09_01_2017_cystic-varigated-submucosal-fibroid_650x450_jpBRADLEY_g_jpg)
Hysteroscopic image of two submucosal fibroids. A 46-year-old woman presented with incessant vaginal bleeding. After undergoing a brief outpatient hysteroscopic myomectomy, her menstrual cycles returned to normal.
Dr. Bradley generally performs six to 10 office hysteroscopies per week. Typical patients may include:
Advertisement
Dr. Bradley also advocates using operative hysteroscopy to remove submucosal and endometrial polyps. “Operative hysteroscopic myomectomy provides excellent outcomes, has low risk of complications and preserves fertility,” she says.
A thorough review of the procedure coauthored by Dr. Bradley was published in Clinical Obstetrics and Gynecology.
“There are so many reasons to make hysteroscopy part of your armamentarium,” she says.
Advertisement
Advertisement

Counseling and careful surgical considerations are key

Deprivation is linked to impaired glucose intolerance and racial disparities

Perioperative prophylaxis and class III obesity

Artesunate ointment is safe well and tolerated patients with vulvar intraepithelial neoplasia

Endoscopic balloon dilation during pregnancy helps optimize outcomes

Researchers examine waste and implore colleagues to take action

Mode of delivery does not affect patient satisfaction