Locations:

Management should focus on improving arc of motion
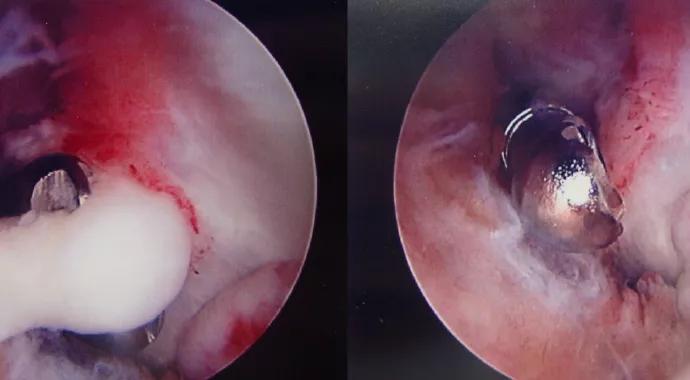
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/fe390a59-d8b3-4e06-b2f8-bfb32dbf4026/Maschke-Hero-Image-690x380pxl_jpg)
Maschke-Hero-Image-690x380pxl
By Nathan G. Everding, MD; Steven D. Maschke, MD; and Peter J. Evans, MD, PhD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Although advances in basic science, rehabilitation protocols and surgical management continue to improve outcomes in patients with elbow stiffness, treatment of elbow contracture remains challenging. Management should focus on improving motion, with the goal of regaining a functional arc of motion. This article summarizes the systematic approach we follow in Cleveland Clinic’s Center for Hand and Upper Extremity Surgery to achieve that goal for as many patients as possible.
The etiology of elbow stiffness is the basis for its classification, diagnosis, prevention and treatment. Traumatic causes of elbow stiffness include fractures, dislocations, crush injuries, burns and head injury. Elective elbow surgery results in controlled trauma to the tissues and may also be complicated by elbow stiffness. Atraumatic causes include rheumatoid arthritis, osteoarthritis, post-septic arthritis, hemophilia-associated hemarthroses, congenital contractures and congenital radial head dislocation. Bone and soft tissue ultimately provide the mechanical blocks to motion that result in elbow stiffness (Figure 1).

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/baec7570-c9b4-498b-9b77-9d8338eae3a8/Maschke-Inset-Image-Figure-1-590pxl-width_jpg)
Figure 1. Thickened contracted capsule viewed during excision from a lateral approach.
Prevention starts with appropriate management of the underlying disease processes to minimize joint destruction. In post-traumatic or postoperative scenarios, early motion protocols are recommended to resolve swelling, maintain motion and prevent contracture. Elbow stability is required for early motion and must be obtained before the patient is taken from the operating room.
Advertisement
Prevention of heterotopic ossification (HO) about the elbow is an additional concern after elbow surgery, trauma or burns. No evidence-based protocols have been defined for managing elbow HO, but the use of indomethacin, which has been proven effective for HO around the hip, has been extrapolated to the elbow. Postoperative radiation therapy for prevention of elbow HO has also been studied recently at Cleveland Clinic1 and is considered functionally beneficial. Following resection of elbow HO, we routinely use indomethacin and radiation therapy in patients with a history of HO. Notably, radiation therapy should not be used acutely after fracture fixation because it has been shown to increase the risk of nonunion.2
Timing, severity, patient-specific factors and underlying pathology guide selection of specific treatment protocols. Following a thorough evaluation that includes history, physical and plain radiographs, a treatment plan can be developed. If further detail of articular surface irregularities or HO is required, CT can be obtained.
Nonoperative treatment is generally considered on initial presentation in patients with minimal contractures of six months’ duration or less. Any treatment protocol should include physical or occupational therapy to optimize outcome, but additional modalities are often necessary. Nonsurgical treatments for elbow stiffness include serial casting, static and dynamic splinting, continuous passive motion, manipulation and botulinum toxin A injections.
Advertisement
Static progressive or dynamic splinting (Figure 2) is a quintessential component of nonoperative management, as it extends the benefits of therapy into daily life. Both methods attempt to achieve plastic deformation of the tissues, leading to remodeling and permanent lengthening. We prefer static progressive splinting because we have observed it to be associated with less discomfort and better compliance; both methods have proven effective in the literature.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/054db8fa-a5b8-45bb-8f1e-b907e21ad5a9/Maschke-Inset-Image-Figure-2-590pxl-width_jpg)
Figure 2. Static progressive elbow splint (left) and dynamic elbow splint (right).
Surgery is appropriate for patients who have not achieved adequate pain relief or functional range of motion after nonoperative management or who have substantial bony blocks.
The decision to operate is based on elbow function and patient factors. Flexion contractures greater than 30° or the inability to flex the elbow to at least 130° is often an indication for surgery. Recent results regarding surgical release demonstrate favorable improvements in elbow motion and function with both open and arthroscopic techniques. All procedures must respect the close proximity of critical neurovascular structures; minimize soft tissue trauma by exploiting defined soft tissue planes and/or intervals; and allow for critical evaluation of fracture reduction, stability and intraoperative gains in range of motion.
The decision to operate is based on elbow function and patient factors. Flexion contractures greater than 30° or the inability to flex the elbow to at least 130° is often an indication for surgery. Recent results regarding surgical release demonstrate favorable improvements in elbow motion and function with both open and arthroscopic techniques. All procedures must respect the close proximity of critical neurovascular structures; minimize soft tissue trauma by exploiting defined soft tissue planes and/or intervals; and allow for critical evaluation of fracture reduction, stability and intraoperative gains in range of motion.
Advertisement
Choice of technique for elbow release starts with determining whether the loss of motion is in flexion, extension or both and whether osteophytes or heterotopic bone contribute. All our patients receive regional neurologic blockade with additional general anesthetic, which varies by procedure and patient. Regional anesthetic is typically an indwelling supraclavicular continuous blockade with a battery pump and refillable reservoir, which has been used for three days to three weeks.
Patients who lack flexion alone have considerable contracture of the posterior band of the medial collateral ligament (pMCL). The pMCL lies on the floor of the cubital tunnel, and excessive scarring can lead to ulnar nerve compression, tethering and subsequent symptoms. If a patient cannot passively flex more than 90° to 100°, we prefer open release of the ulnar nerve and resection of the pMCL and medial joint capsule. The remainder of the release and posterior capsulectomy are then performed open through the same incision ‒ which is safe, reliable and efficient ‒ and the ulnar nerve is transposed subcutaneously. There is no tendon healing, so scar formation is minimal and arthroscopic release offers little advantage.
If a patient has acceptable flexion and lacks only extension, the release can be done either all arthroscopically or open via the lateral column or a medial over-the-top technique. We prefer an arthroscopic release (Figure 3) of the anterior elbow to gain extension, as it avoids tendon healing and minimizes postoperative scar formation.
Advertisement

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/84ba55b9-e1eb-4bbb-bdea-f0c7b9d463ef/Maschke-Inset-Image-Figure-3-590pxl-width_jpg)
Figure 3. Arthroscopic view of an elbow with abundant soft tissue adhesions (left). Arthroscopic lysis of adhesions (middle) and debridement (right).
For patients with combined flexion and extension contractures but with more than 100° of flexion, the ulnar nerve does not require release and capsular resection alone may restore all motion; in these cases, technique (open or arthroscopic) comes down to surgeon preference. However, the surgeon should be prepared to perform an adjuvant open medial incision to resect the pMCL if adequate flexion is not achieved.
For patients with combined flexion and extension contractures with less than 90° of flexion, the preceding considerations apply, and we prefer arthroscopic release of the anterior elbow combined with open medial and posterior release of the elbow with ulnar nerve transposition. The ulnar nerve is exposed first and decompressed in the cubital tunnel and flexor forearm muscles. It is left undisturbed proximal to the medial epicondyle, as this allows the medial intermuscular septum to protect the nerve when the superior-medial portal is used. The anterior elbow is then arthroscopically released and the ulnar nerve is released proximally; the intermuscular septum, pMCL, and medial and posterior joint capsule are resected through the existing medial incision; and the nerve is transposed subcutaneously. Again, this avoids tendon healing and minimizes scar formation. When heterotopic bone needs to be removed, we prefer open resection only, and often simultaneous open medial and lateral approaches.3,4
Postoperatively, the elbow is splinted in extension for 24 hours, to rest the tissues and minimize bleeding and subsequent swelling. The splint is removed and activities of daily living are commenced after placement of a compression dressing. Ice or a compression ice system is used 20 minutes every one to two hours for the first 72 hours with hand squeezing of a light compression foam block to augment venous and lymphatic return. If insurance allows, continuous passive motion for flexion-extension (and pronationsupination, if required) is begun in the patient’s home after 72 hours. After six weeks, static progressive splinting may be started to increase motion. Night splinting in either flexion or extension (to counter the larger deficit) is continued.
Based on feedback from the therapists and re-examination, we will consider manipulation under anesthesia, botulinum toxin A injection (biceps and brachialis) and intra-articular injection of a corticosteroid within the first three weeks. Exercises, splinting and therapy are maintained until a plateau is reached, with the expectation that gains can continue for up to 12 months.
1. Robinson CG, Polster JM, Reddy CA, et al. Postoperative single-fraction radiation for prevention of heterotopic ossification of the elbow. Int J Radiat Oncol Biol Phys. 2010;77(5): 1493-1499.
2. Hamid N, Ashraf N, Bosse MJ, et al. Radiation therapy for heterotopic ossification prophylaxis acutely after elbow trauma: a prospective randomized study. J Bone Joint Surg Am. 2010;92(11):2032-2038.
3. Evans PJ, Nandi S, Maschke S, Hoyen HA, Lawton JN. Prevention and treatment of elbow stiffness. J Hand Surg Am. 2009;34(4):769-778.
4. Nandi S, Maschke S, Evans PJ, Lawton JN. The stiff elbow. Hand (N Y). 2009;4(4):368-379.
Dr. Everding is a fellow with the Cleveland Combined Hand Fellowship.
Dr. Maschke is a hand, wrist and elbow surgeon in the Department of Orthopaedic Surgery and a staff member with the Cleveland Combined Hand Fellowship.
Dr. Evans is Director of the Center for Hand and Upper Extremity Surgery in the Department of Orthopaedic Surgery. He is also Director of the Cleveland Combined Hand Fellowship.
Advertisement

Biologic approaches, growing implants and more

Study reports zero infections in nearly 300 patients

How to diagnose and treat crystalline arthropathy after knee replacement

Study finds that fracture and infection are rare

Center will coordinate, interpret and archive imaging data for all multicenter trials conducted by the foundation’s Osteoarthritis Clinical Trial Network

Reduced narcotic use is the latest on the list of robotic surgery advantages

Cleveland Clinic specialists offer annual refresher on upper extremity fundamentals

Cleveland Clinic orthopaedic surgeons share their best tips, most challenging cases and biggest misperceptions