Locations:

Is there a risk?

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/dbaf67e6-4335-4e40-90a6-edb8d6d6d19c/DPP-4_650x450_jpg)
DPP-4_650x450
Three randomized controlled clinical trials evaluating the cardiovascular safety of dipeptidyl peptidase (DDP)-4 inhibitors suggest this class of drugs is neutral in terms of myocardial infarction and death.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
But saxagliptin was found to have a small increased risk for hospitalization for heart failure in one study. And a Cleveland Clinic retrospective review found a slight increased risk of heart failure when DPP-4 therapy was added to metformin.
The Saxagliptin Assessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus (SAVOR)-Thrombolysis in Myocardial Infarction (TIMI) 53 trial, published in 2013 in the New England Journal of Medicine, found that while saxagliptin improves glycemic control, hospitalization rates for heart failure increased.
SAVOR TIMI 53 found saxagliptin caused an unexpected 27 percent increase in the relative risk of hospitalization for congestive heart failure (CHF) (hazard ratio, 1.27; 95 percent CI, 1.07 to 1.51; P = 0.007). The largest number of increased hospitalizations occurred among patients with baseline blood levels of NT-pro-brain natriurectic peptide of at least 333 pg/mL. The greatest excess rate of hospitalization for heart failure occurred within the first six months of treatment. After that, hospitalization rates for heart failure were virtually identical in the two treatment arms of the study.
The examination of Cardiovascular Outcomes with Alogliptin versus Standard of Care (EXAMINE) trial, published in 2013 in the New England Journal of Medicine, did not find increased rates of major adverse cardiovascular events, nor a significant increased risk of CHF admissions, with alogliptin. However, there was an increase in the number of patients admitted with heart failure.
Advertisement
The Trial Evaluating Cardiovascular Outcomes with Sitagliptin (TECOS), published in 2015, similarly did not find an increased risk of major adverse cardiovascular events or hospitalization for heart failure by adding sitagliptin to treatment.
Although EXAMINE and TECOS did not duplicate SAVOR TIMI 53 findings, these results raised concern regarding the risk of CHF with DPP-4 therapy, particularly since this class of drugs is routinely used in clinical practice post-approval in high-risk cardiovascular patients because of these drugs’ previously perceived cardiovascular safety.
Because of these findings, we sought to evaluate the risk of CHF among patients who received metformin, the recommended first-line agent to control glycemia in patients with type 2 diabetes (T2D), in combination with a DPP-4 versus in combination with the other commonly utilized second-line anti-diabetic agents (sulfonylurea, thiazolidinedione and glucagon-like peptide [GLP]-1 agonists).
A retrospective cohort study was conducted using our enterprise-wide electronic health record (EHR) system to identify 13,185 patients with T2D seen in the outpatient clinics who received a prescription for metformin in combination with a sulfonylurea (N = 9,419), thiazolidinedione (N = 1,846), DPP-4-I (N = 1,487) or a GLP-1 receptor agonist (N = 433), seen in the outpatient clinics who were at least 18 years of age; who had no history of CHF or coronary artery disease; and were not using insulin or undergoing dialysis at baseline. The patients were followed for CHF by documentation in the EHR. Cox multiple regression models were used to compare cohorts. Combination therapy with metformin and sulfonylurea served as the comparator group.
Advertisement
Baseline characteristics for the entire cohort included mean (± SD) age 60.6 ± 12.6 years, 54.6 percent male and 75.8 percent Caucasian. The median follow-up was four years. There were 528 CHF events in 55,110.76 person years of follow-up. A higher risk of CHF was observed with metformin and DPP-4-I use
(HR 1.104; 95% CI, 1.04-1.17; P = 0.001), but so too was a trend toward a statistically significant increased risk with other combinations: metformin and thiazolidinedione (HR 1.024; 95% CI, 0.98-1.07) and metformin and a GLP-1 receptor agonist (HR 1.1; 95% CI, 0.99-1.22).
Based on EXAMINE and SAVOR TIMI 53, the FDA recently issued a warning regarding a small, increased risk of heart failure in patients treated with saxagliptin and alogliptin, but not sitagliptin. The FDA warning for saxagliptin and alogliptin is consistent with our retrospective review.
The significance of the SAVOR TIMI 53 findings is unclear given it was not observed in the other DDP-4 inhibitor cardiovascular safety trials. It is not clear if this finding is related to differences in study design, slightly different study populations, a problem specific to saxagliptin, or possibly statistical chance. Further investigation of this finding with saxagliptin is necessary.
Our results and those of SAVOR TIMI 53— while interesting and hypothesis-generating— should not result in a total abandonment of DPP-4 use.
Overall, the available evidence suggests that the DPP-4 inhibitor class of drugs is neutral, in terms of cardiac safety. This finding, and the drugs’ other recognized benefits – avoiding hypoglycemia and weight gain – should be considered when a clinician is choosing an oral anti-hyperglycemic agent.
Advertisement
Kevin M. Pantalone, DO, is an endocrinologist in the Department of Endocrinology, Diabetes and Metabolism and Director of Clinical Research. He can be reached at 216.445.9060 or pantalk@ccf.org.
Robert S. Zimmerman, MD, is Vice Chairman of the Department of Endocrinology, Diabetes and Metabolism and Director of Cleveland Clinic’s Diabetes Center. Contact him at 216.444.9428 or zimmerr@ccf.org.
Disclosure: Drs. Pantalone and Zimmerman have received research funding and consulting and speaking compensation from Merck and Novo Nordisk within the past 12 months. In addition, Dr. Pantalone has received compensation from Astrazeneca for serving as a speaker and from Eli Lilly for serving as a consultant.
Advertisement
Advertisement

Radiofrequency ablation significantly reduces symptom severity, shrinks nodules

Maternal-fetal medicine specialists, endocrinologists and educators team up

Giving young patients a hand as they take charge of their own health

Case illustrates how easily condition can mimic preeclampsia
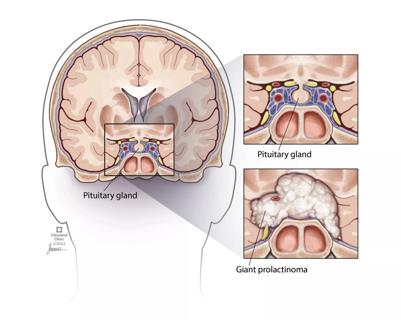
Analysis examines surgical resection of rare pituitary tumors
Screening and medication key to better outcomes

Spinal cord stimulation can help those who are optimized for success
Incidence, outcomes and management