Locations:

Study shows how idiosyncratic dose-response patterns can be

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/2b9e79cf-1c3e-4dbf-9fa8-1adafd35ce69/15-NEU-2530-Manos-650x450_jpg)
15-NEU-2530-Manos-650×450
By Michael Manos, PhD; Eric Geyer, BA; Ralph D’Alessio, BA; Kimberly Giuliano, MD; and Michael Macknin, MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Substantial evidence from clinical trials confirms that psychostimulants improve symptoms in children with attention deficit hyperactivity disorder (ADHD) and that their pharmacokinetic properties are well-documented.1
There remains, however, a dearth of information on how behavior changes during stimulant titration.
The prescribe-and-wait method, in which the physician uses the skill and art of medical practice to determine the best dose, is common and may be informed only by the physician’s personal experience with patients.2 In clinical practice, however, stimulant dose response varies considerably across ADHD subtypes, patient age and gender, type of stimulant, and other variables that have been only peripherally studied.3
To date, factors that inform and predict response to stimulants remain elusive. Because the relationship between dose and response tends to be predominantly linear (as dose increases, behavioral improvement increases), clinicians have a tendency to expect this pattern and subsequently may not systematically observe and measure response as it occurs. Response variability often goes unnoticed,4 and when it is overlooked, optimal treatment can be compromised.
Early clinical practice parameters suggested that dosing should be carried out according to gross body weight, beginning with 0.3 mg/kg in a twice-daily regimen and titrated upward until undesirable side effects emerged or behavior improved. This method was untenable, however, because pharmacological factors such as drug absorption, metabolism and excretion rates produce great interindividual variability.5
Advertisement
Although a linear dose response is found consistently at the group level of analysis, individual children vary considerably in behavior change across dose levels.6 In addition to a linear response, there are five other patterns of response in individuals:
Three curves are predictable in that they tend to yield results in specific regimens and have a readily recognizable course of action. Behavior that improves as dose increases (linear response) indicates to the physician that an optimal dose may be achieved by ramping up the dose. If behavior deteriorates at higher doses (curvilinear response), the best dose is achieved by using the dose just prior to deterioration. If no response is observed at the initial doses, a further increase in dose may still yield optimal response (threshold response).
The remaining three curves, however, are unpredictable and do not help guide the physician’s next action during titration. Curves that inconsistently improve response despite increase or decrease in dose (variable response) give little guidance as to the next action, such as to terminate, change or extend the titration. The same case applies when individuals respond to treatment regardless of the medicine or dose (placebo response). Finally, some children do not respond to medicine except at unusual dose levels (no change), and these cases are seldom pursued in primary care. Dose curves are illustrated in the figure.
Advertisement
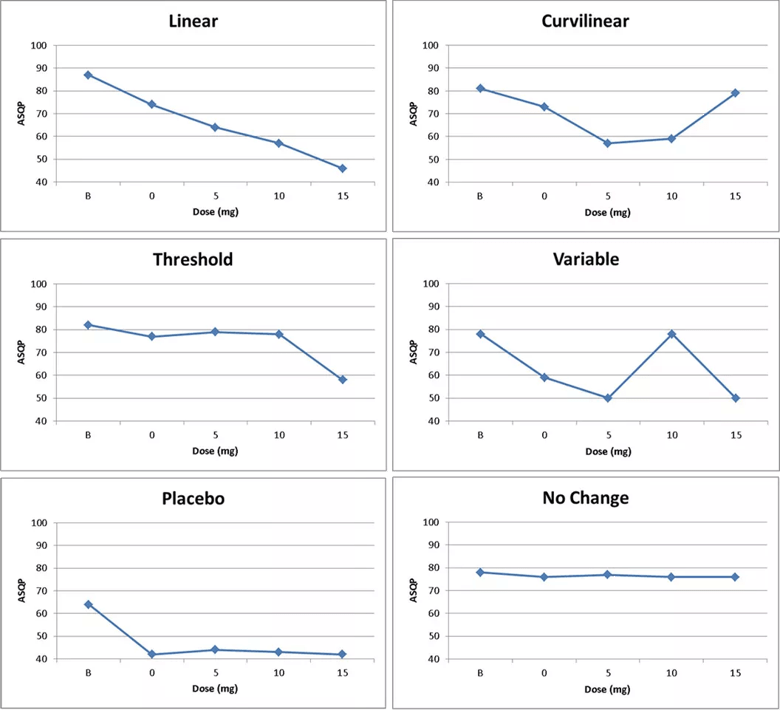
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/62567f2e-ec61-440a-a1fb-8b90b96caae1/15-NEU-2530-Inset_png)
Figure. Six dose-response curves from a sample of youths ages 5 to 17 prescribed methylphenidate, mixed amphetamine salts (MAS) or sculpted dosing of MAS (see main text) in Cleveland Clinic’s ADHD Medication Monitoring Clinic. A lower score indicates symptom reduction. ASQP = Abbreviated Symptom Questionnaire for parents. The dose response of the 249 youths was as follows: linear, n = 106; curvilinear, n = 65; threshold, n = 18; variable, n = 19; placebo, n = 21; no change, n = 20.
These distinctions describe dose-response patterns that confound titration of psychostimulants during pharmacotherapy for children with ADHD. They also identify characteristic patterns with implications for pediatric practice for ADHD treatment. We investigated these patterns in the Medication Monitoring Clinic of Cleveland Clinic’s ADHD Center for Evaluation and Treatment.
A sample of 249 youths meeting DSM-III or DSM-IV diagnostic criteria for ADHD was evaluated using a four-week, double-blind, placebo-controlled protocol. Physicians prescribed twice-daily dosing of methylphenidate, once-daily dosing of mixed amphetamine salts (MAS) or sculpted dosing of MAS (higher dose in the morning, 5-mg dose at about 3 p.m.) for youths ages 5 to 17 years. Data were collected at baseline and across the pharmacological protocol, which specified four possible dosing sequences (BL = baseline, A = placebo, B1 = 5 mg, B2 = 10 mg, B3 = 15 mg):
Each participant was randomized to one of the four sequences. Teachers and parents rated symptom presence at baseline and at the end of each treatment week using the Conners Abbreviated Symptom Questionnaire for parents.7
Advertisement
Children’s responses to individual psychostimulant medications varied by age. Predictable dose-response curves (linear, curvilinear and threshold) were associated with younger children (< 10 years), and unpredictable curves (variable, no response and placebo) were associated with older children (> 9 years). The idiosyncratic nature of children’s responses to psychostimulants requires close monitoring during titration to optimize treatment. These results underscore the need to use more sophisticated dosing strategies at older ages.
Advertisement
Dr. Manos is Director of Cleveland Clinic’s Center for Pediatric Behavioral Health.
Mr. Geyer is a psychometrist and Mr. D’Alessio a clinical research assistant, both in the Center for Pediatric Behavioral Health.
Drs. Giuliano and Macknin are staff physicians in the Department of General Pediatrics.
Advertisement

New study advances understanding of patient-defined goals

Testing options and therapies are expanding for this poorly understood sleep disorder

Real-world claims data and tissue culture studies set the stage for randomized clinical testing

Digital subtraction angiography remains central to assessment of ‘benign’ PMSAH

Cleveland Clinic neuromuscular specialist shares insights on AI in his field and beyond

Findings challenge dogma that microglia are exclusively destructive regardless of location in brain

Neurology is especially well positioned for opportunities to enhance clinical care and medical training

New review distills insights from studies over the past decade