Locations:

Endovascular procedures associated with lower mortality, LOS, cost vs. surgical bypass
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/2e6eae1b-fd8b-4fe5-8c32-e356850cbc1c/16-HRT-287-Shishebor-Hero-Image_jpg)
Critical Limb Ischemia
Recent years have seen progress in combating critical limb ischemia (CLI) in the United States, but the progress has been mixed and appears to be driven by increasing numbers of minimally invasive percutaneous (endovascular) procedures.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
So suggests a new comprehensive analysis of a nationwide hospital sample of nearly 650,000 patients conducted from 2003 to 2011.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/0cd04e76-8e65-400e-a7e3-7659a6d4defb/16-HRT-287-Shishebor-Inset-Portrait_jpg)
Mehdi Shishehbor, DO, MPH, PhD
“We found that rates of surgery for CLI are going down while rates of endovascular procedures are going up,” says Mehdi Shishehbor, DO, MPH, PhD, Director of Endovascular Services at Cleveland Clinic. “Meanwhile hospital admissions for CLI have remained constant even as rates of amputation and death from CLI have gone down. This suggests there’s something at work other than improved medical therapy for CLI.”
Dr. Shishehbor led the Cleveland Clinic-conducted analysis, which was just published in Journal of the American College of Cardiology and will also be presented at the 65th Annual Scientific Session of the American College of Cardiology (ACC.16) in Chicago in early April.
CLI — defined as the presence of ulcers, gangrene or rest pain plus peripheral artery disease (PAD) — affects an estimated 10 million U.S. adults and is a major cause of pain, immobility, diminished quality of life, amputation and death.
A significant rise in endovascular revascularization as a treatment for CLI, accompanied by a decrease in surgical revascularization, prompted Dr. Shishehbor and his colleagues to undertake their analysis to more closely examine this trend and its potential associations with changes in CLI outcomes and resource utilization.
They obtained their data from the federal government’s Nationwide Inpatient Sample for 2003-2011, which contains discharge-level data from some 8 million hospitalizations annually across more than 1,000 hospitals. The database is designed to represent a 20 percent stratified sample of all U.S. hospitals.
Advertisement
They identified 642,433 admissions with CLI during this period and assessed these admissions for two primary end points, in-hospital mortality and amputation, as well as two secondary end points, length of stay (LOS) and hospitalization cost.
The researchers’ key findings are reflected in the figure below and include the following:
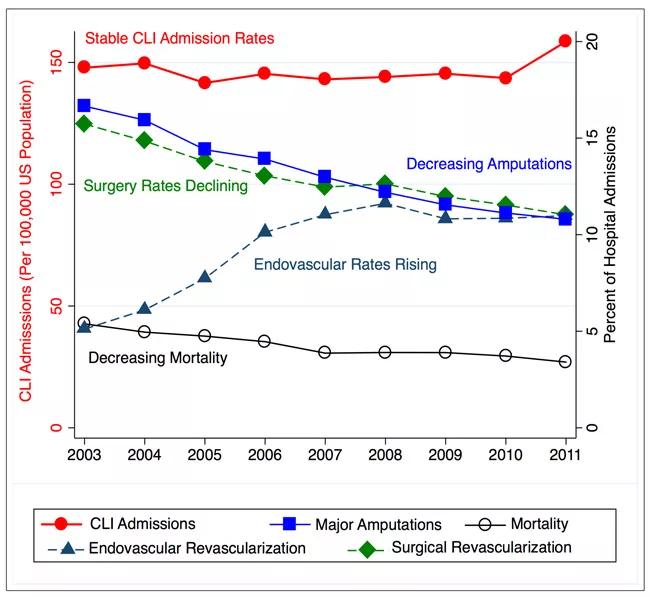
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/2e403bd8-e48b-47e1-87a7-8626e65002f9/16-HRT-287-Shishebor-Inset-Image-650pxl-width_jpg)
Figure. Nationwide trends in CLI hospital admissions and outcomes over time, based on the analysis by Shishehbor and colleagues. Reprinted from Agarwal S, Sud K, Shishehbor MH, J Am Coll Cardiol. 2016 Mar 21 [Epub ahead of print], ©2016, with permission from the American College of Cardiology Foundation.
Advertisement
“We found that endovascular procedures were associated with lower mortality, lower cost and lower length of stay compared with surgical revascularization in this large cohort of patients with CLI,” says Dr. Shishehbor. “While we cannot say it’s causation, these findings imply that endovascular treatment appears to be safer and less costly than surgical procedures for these patients.”
When asked what surprised him most about the study’s findings, Dr. Shishehbor points to the constant rate of patients admitted with CLI throughout the nine-year period.
“We had thought the decrease in amputation and mortality over time was a result of improving medical therapy, but that would lead you to expect a decrease in CLI admissions over time, which didn’t happen,” he explains. “Of course, good medical therapy is extremely important, but the data suggest that good medical therapy needs to be combined with our increasingly effective use of endovascular procedures to make further progress in CLI outcomes.”
Dr. Shishehbor can be reached at 216.636.6918 or shishem@ccf.org.
Advertisement
Advertisement

A sampling of outcome and volume data from our Heart & Vascular Institute

Concomitant AF ablation and LAA occlusion strongly endorsed during elective heart surgery

Large retrospective study supports its addition to BAV repair toolbox at expert centers

Young age, solid tumor, high uptake on PET and KRAS mutation signal risk, suggest need for lobectomy

Surprise findings argue for caution about testosterone use in men at risk for fracture

Residual AR related to severe preoperative AR increases risk of progression, need for reoperation

Findings support emphasis on markers of frailty related to, but not dependent on, age

Provides option for patients previously deemed anatomically unsuitable