Locations:

Retrospective data from 110 patients support use
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/b6343d40-fe5b-4f8a-8dcf-cc68471b67ee/Pathology-Slide_Langford_Hoffman_690x380pxl_jpg)
Pathology Slide_Langford_Hoffman_690x380pxl
By Lama Azar, MD; Jason Springer, MD; Carol A. Langford, MD, MHS; and Gary S. Hoffman, MD, MS, MACR
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Rituximab (RTX) is an effective remission-inducing agent in granulomatosis with polyangiitis (GPA; Wegener’s). It is uncertain whether RTX is best used with or without a conventional agent for remission maintenance. To explore this question, Cleveland Clinic’s Center for Vasculitis Care and Research conducted a single-center retrospective study to assess the efficacy and safety of RTX induction therapy in patients in whom RTX was used alone vs. in combination with a conventional maintenance agent.
We retrospectively analyzed data on all patients with GPA treated by our center with at least one course of RTX (four weekly doses of 375 mg/m2 IV, or two fixed doses of 1,000 mg IV two weeks apart) until November 2011. Remission was defined as a Birmingham Vasculitis Activity Score (modified for Wegener’s) of 0.
Results
In all, 110 patients (median age, 50 years; 51 percent women) were included (Figure 1). In 91 percent, the indication for the first RTX infusion was relapsing or persistent disease. Median follow-up was 23 months (interquartile range [IQR], 10-50).
Complete remission was achieved in 97 percent of patients. Relapses occurred in 47 percent, and the median time to relapse was 13 months (IQR, 7-20.5). Within a subset of 16 patients who were relapse-free at two years after one RTX course, remissions endured for two to six years in eight patients.
Relapse-free survival was significantly higher in patients receiving a conventional maintenance agent (azathioprine [AZA], methotrexate [MTX] or, if AZA or MTX were not tolerated, mycophenolate mofetil [MMF]) in conjunction with RTX and glucocorticoids (n = 49) than in those not receiving a maintenance agent (n = 43) (P = .04) (Figure 2). The hazard ratio for relapse was 0.54 (95% confidence interval, 0.30-0.99) in those receiving a second agent for remission maintenance.
Advertisement
Serious adverse events did not differ between the two groups.
Implications Until Prospective Trials Are Performed
Addition of a conventional maintenance agent to RTX and glucocorticoids reduced the incidence of GPA relapse without resulting in a higher incidence of adverse events. Prospective trials comparing conventional immunosuppressive maintenance agents with repeated scheduled RTX doses are needed.
Until those data are available, our findings support the addition of a conventional maintenance agent (AZA or MTX), in the absence of contraindications or intolerance, to reduce the risk of GPA relapse.
This research was originally presented by Dr. Azar at the 2012 American College of Rheumatology Annual Meeting.
Dr. Azar completed a rheumatology fellowship in the Department of Rheumatic and Immunologic Diseases in 2013.
Dr. Springer completed a vasculitis fellowship in the Department of Rheumatic and Immunologic Diseases in 2013.
Dr. Langford is Director of the Center for Vasculitis Care and Research as well as Vice Chair for Research, Department of Rheumatic and Immunologic Diseases. She can be reached at langfoc@ccf.org or 216.445.6056.
Dr. Hoffman is a member of the Department of Rheumatic and Immunologic Diseases and the Center for Vasculitis Care and Research.
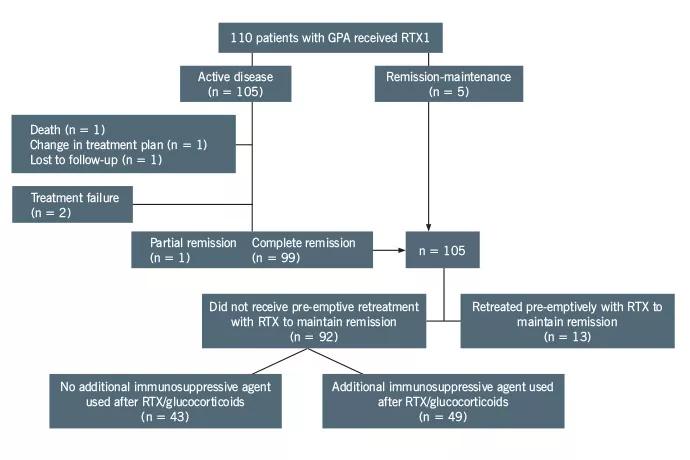
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/418cb47d-b27d-4a10-8f16-efe13f7e084e/Flow-Chart_Fig-1_Hoffman_Langford_690pxl-width_jpg)
Figure 1. Disease course and additional therapies after the first RTX treatment (RTX1). The additional immunosuppressive agent used was either azathioprine (AZA), methotrexate (MTX) or, if AZA or MTX were not tolerated, mycophenolate mofetil (MMF).
Advertisement
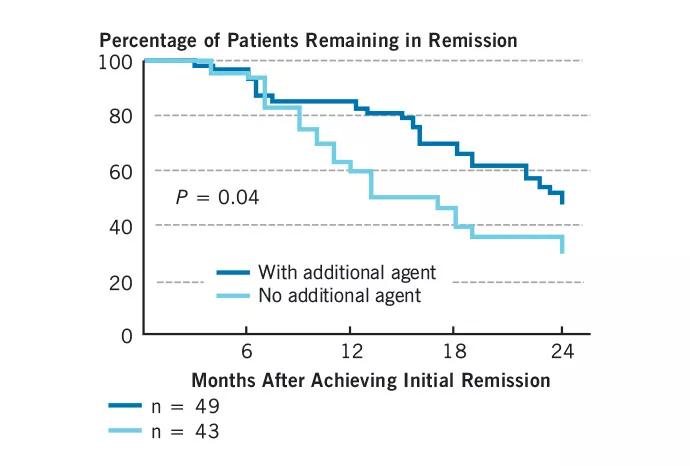
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/b07c87a0-d8cc-4c72-a821-f1562b7869ee/Chart_Fig-2_Hoffman_Langford_690pxl-width_jpg)
Figure 2. Kaplan-Meier analysis showing relapse-free remission in patients treated with RTX and glucocorticoids only (light blue line) vs. patients treated with RTX and glucocorticoids plus an additional immunosuppressive agent (dark blue line). The additional agent was either MTX (n = 12), AZA (n = 29) or MMF (n = 8) (see Figure 1 for abbreviation expansions).
Advertisement
Advertisement
Treatment strategies require understanding of pathomechanisms

Education, prevention strategies and monitoring serves this at-risk group

Treatment for scleroderma can sometimes cause esophageal symptoms

Lupus Clinic providers collaborate to advance treatment and understanding

Older Psoriasis Patients May Experience Quicker Transition

Cleveland Clinic’s Rheumatic Lung Disease program treats patients with complex conditions

Symptoms complement one another

E-coaching program is tailored for those with the disease