Locations:

Diagnosis confirmed as rare antisynthetase syndrome

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/a447e0fb-cec6-4c10-8831-e9f45cc725c7/Chatterjee-Hero-Image-690x380pxl_jpg)
Chatterjee-Hero-Image-690x380pxl
By Soumya Chatterjee, MD, MS, FRCP, FACP, FACR
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
A 66-year-old man was initially seen in our rheumatology clinic with a five-month history of polyarthralgia associated with swollen fingers, wrists and knees as well as significant early-morning stiffness. He also developed progressive proximal myopathy. He had no fever, chills, headaches, dysphagia or sicca symptoms. In a few months, he developed progressive shortness of breath on exertion and a nonproductive cough.
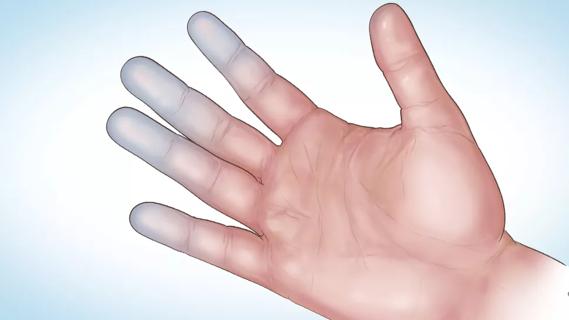
He had a positive ANA (5.7 OD ratio [normal, < 1.5]) and a positive Jo-1 antibody (antibody to histidyl transfer RNA synthetase). His creatine kinase was 700 U/L (normal, 30-220). EMG was consistent with a necrotizing myopathy. On pulmonary function testing, his forced vital capacity was 80 percent of predicted and his carbon monoxide diffusing capacity was 67 percent of predicted. Thoracic high-resolution CT scan revealed evidence of interstitial lung disease (ILD) characterized by bilateral patchy ground-glass opacities suggestive of active alveolitis, most extensive at the lung bases (Figure 1). A few months later, the skin of the tips and radial margins of his fingers started thickening and cracking, matching the classic description of “mechanic’s hands.”

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/ffb711c9-eacd-4414-9ff7-a1e095f4635a/Chatterjee-Inset-590-pxl-width_jpg)
Figure 1. Thoracic high-resolution CT scan in a 66-year-old man with interstitial lung disease and fibrosis associated with antisynthetase (anti-Jo-1) syndrome. Note the bilateral patchy ground-glass opacities suggestive of active alveolitis, most extensive at the lung bases, along with bilateral subpleural reticular infiltrates and interlobular septal thickening.
Advertisement
The patient was seen in our combined rheumatology/pulmonary clinic and bronchoscopy was arranged. Bronchoalveolar lavage indicated alveolitis with pathologic changes on biopsy consistent with organizing pneumonia. All cultures were negative. The constellation of manifestations, including inflammatory muscle disease, ILD, mechanic’s hands and inflammatory polyarthritis, along with positive antibodies to histidyl transfer RNA synthetase (Jo-1 antibody), confirmed the diagnosis of antisynthetase syndrome.
The patient was started on daily oral cyclophosphamide along with high-dose oral prednisone. The dose of cyclophosphamide was gradually increased with close monitoring of his complete blood count. There was substantial improvement in proximal muscle strength, and his creatine kinase normalized (66 U/L) in a few months. However, the cyclophosphamide dose had to be further increased because repeat bronchoscopy still showed active alveolitis. Subsequently, his ILD improved and his exertional dyspnea, pulmonary function test results and thoracic high-resolution CT scan all showed significant improvement. Because his condition was in remission, cyclophosphamide was discontinued after 12 months and he was started on a maintenance immunosuppressive regimen of oral methotrexate 15 mg weekly along with prednisone.
This case is a good example of high-complexity medical decision-making. It should be recognized that important and often lifesaving management decisions about rare and complex conditions such as this frequently have to be based on expert opinions alone, as well-designed randomized controlled trials are often not available. It is imperative that cases like this be managed jointly by a rheumatologist and a pulmonologist.
Advertisement
Our combined rheumatology/pulmonary clinic makes such close collaboration possible. In this clinic, decisions about the investigation and management of complicated cases like this can be made in conjunction by two different subspecialists who can combine their respective perspectives. Patients appreciate getting collaborative opinions about their care from specialists with distinct areas of expertise who are experienced in managing different aspects of their disease. Moreover, rheumatology trainees benefit from the unique opportunities to learn about the methods involved in such complex decision making and from the abundant opportunities for fellowship research projects.
Dr. Chatterjee runs Cleveland Clinic’s rheumatology/pulmonary clinic with staff pulmonologist Joseph Parambil, MD, who has a special interest in autoimmune rheumatic disease-associated interstitial lung disease and pulmonary hypertension. This clinic integrates evidence-based care with clinical and translational research on the complex pathogenesis and management of rheumatic diseases affecting the lung.
Advertisement
Advertisement
Treatment strategies require understanding of pathomechanisms

Education, prevention strategies and monitoring serves this at-risk group

Treatment for scleroderma can sometimes cause esophageal symptoms

Lupus Clinic providers collaborate to advance treatment and understanding

Older Psoriasis Patients May Experience Quicker Transition

Cleveland Clinic’s Rheumatic Lung Disease program treats patients with complex conditions

Symptoms complement one another

E-coaching program is tailored for those with the disease