Locations:

Case shows feasibility of using robot for complex urologic reconstruction

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/9e83dd45-cc4f-4f13-9100-f2f35d417176/15-URL-057-Kaouk-Hero-Image-690x380pxl_jpg)
15-URL-057-Kaouk-Hero-Image-690x380pxl
By Jihad Kaouk, MD; Dinesh Samarasekera, MD; Christopher Starks, MD; and Edmund Sabanegh Jr., MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Microsurgical vasectomy reversal can be technically challenging. We have performed robot-assisted vasovasostomy via a scrotal incision. The procedure may offer some advantage, including elimination of surgeon tremor and decreased surgeon fatigue. Here, we present a unique case of a transabdominal robot-assisted laparoscopic vasovasostomy.
A 34-year-old male underwent a transabdominal vasectomy at the time of a diagnostic laparoscopy for evaluation of inguinal hernias. He presented post-vasectomy with chronic bilateral orchalgia, which was unresponsive to analgesia. The patient had been evaluated by the chronic pain service and had no resolution of his symptoms. He was diagnosed with post-vasectomy pain syndrome and referred for a vasectomy reversal.
The patient had three children with his current partner, and the couple was now interested in additional children. His body mass index was 27.67 kg/m2, and his past surgical history included the diagnostic laparoscopy/vasectomy and a laparoscopic cholecystectomy. A urinalysis was negative. We presented all options to the patient, and the decision was made to proceed with a robot-assisted laparoscopic vasovasostomy.
We placed the patient in the lithotomy position, in steep Trendelenberg. Port placement was similar to that of a radical prostatectomy, in a W configuration. We docked the robot between the patient’s legs in a standard fashion. We removed the surgical clips on each vas, and performed the vasovasostomy with a 9-0 monofilament suture using a modified two-layer technique that involved quadrant full-thickness luminal stitches and additional interrupted seromuscular stitches after we documented patency (Figure 1).
Advertisement
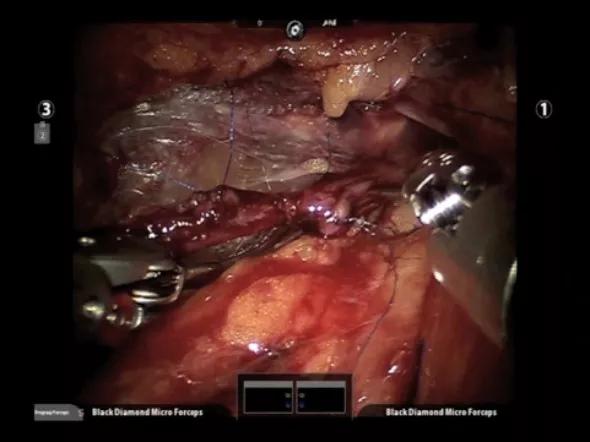
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/0a165fec-c4e6-4a8c-94c7-e65e5728313d/04-Inset-Image-590pxl-width_jpg)
Figure 1. Vasovasostomy performed with 9-0 monofilament suture.
Operative time was 300 minutes, and estimated blood loss was less than 50 cc. There were no intraoperative complications. The patient was discharged to home the same day.
Semen analysis six months post-procedure revealed normal volume and concentration but 99 percent immotility. Anti-sperm antibody testing was positive, and the patient is being treated with steroid therapy. He has had complete resolution of his post-vasectomy pain syndrome.
Transabdominal vasovasostomy is technically feasible. This represents a unique case, as most vasectomies are not done in a transabdominal fashion. However, this demonstrates the ability to perform complex reconstructive procedures robotically. Advantages include elimination of surgeon tremor, excellent visualization, and precise dissection and suturing with robotic micro instruments in the peritoneal cavity.
Dr. Kaouk is Director of Cleveland Clinic Glickman Urological & Kidney Institute’s Center for Robotic and Laparoscopic Surgery and is the Urological & Kidney Institute’s Vice Chair for Surgical Innovations. He is a Professor of Surgery at Cleveland Clinic Lerner College of Medicine.
At the time this article was written, Drs. Samarasekera and Starks were Clinical Fellows at the Urological & Kidney Institute.
Dr. Sabanegh is Chairman of the Urological & Kidney Institute’s Department of Urology.
Advertisement
Advertisement

Clinicians should individualize dosing practices based on patient risk factors and preferences
Pioneering and refining the approach in pyeloplasty, nephrectomy and more
Fully-automated process uses preop CT, baseline GFR to estimate post-nephrectomy renal function

Could mean earlier treatment, but also could have negative effects

Unlike earlier pills, new drugs do not cause liver toxicity

Male factors play a role in about half of all infertility cases, yet men often are not evaluated
Surgeons choreograph nearly simultaneous procedures, sharing one robot between two patients

Identifying barriers in the renal genetic assessment of Black patients