Locations:

Weighing the conduit options means balancing a host of factors
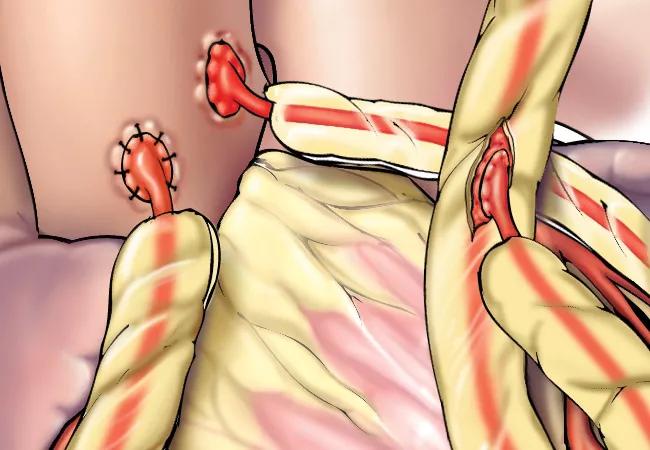
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/d27f1ea4-a41e-42bc-8355-d1f518ddb02c/15-HRT-3041-Artierial-Graft-CQD-650x450_jpg)
Arterial Graft
Coronary artery bypass grafting (CABG) remains the gold-standard treatment for coronary artery disease. But which grafts are best for bypass surgery?
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
The choice of bypass graft depends on a number of factors:
The success of CABG depends on the long-term patency of the arterial or venous grafts used, notes Michael Zhen-Yu Tong, MD, MBA, a cardiac surgeon in Cleveland Clinic’s Department of Thoracic and Cardiovascular Surgery. “In general, arterial grafts are better and more durable than veins,” he says, pointing out that arterial grafts are considered superior conduits over saphenous vein grafts based on experience using the left internal mammary artery to bypass the left anterior descending (LAD) coronary artery. The efficacy of the radial artery graft is less clear, he adds.
Consult QD recently caught up with Dr. Tong for the following summary of pros and cons of various artery and vein graft options in CABG procedures.
As the most commonly used bypass grafts, the internal thoracic (mammary) artery (ITA) grafts show the best long-term results. In most cases, the artery is left intact at its origin, with the opposite end sewn to the coronary artery below the site of the blockage. Use of ITA grafts is considered a quality indicator by the Society of Thoracic Surgeons (STS) and is factored into STS star-rating calculations for cardiac surgery programs. “We aim to use at least one ITA graft in 100 percent of patients undergoing isolated coronary bypass surgery,” Dr. Tong notes.
ITA grafts are resistant to late failure. Studies of angiograms performed after bypass surgery show that not only do left ITA-LAD grafts have a more than 90 percent chance of functioning well early, but these grafts continue to function well over the long term. Development of obstructions in these grafts has been shown to be extremely uncommon.
Advertisement
Long-term follow-up studies done at Cleveland Clinic from the 1980s showed that these grafts have an important long-term effect on clinical outcomes. Over time, patients with left ITA-LAD grafts were less likely to die or need reoperation compared with patients who received only vein grafts. This is now a standard for coronary bypass grafting.
In addition to the left ITA, the right ITA is also often used in patients age 65 or younger — and also in older but otherwise relatively healthy patients when more than one graft is needed, says Dr. Tong. Long-term studies from Cleveland Clinic found that bilateral ITA grafts further decrease the long-term risks of death and reoperation compared with single ITA grafts. Use of both ITAs as bypass grafts is more complex and is not appropriate for some patients.
“When more than one graft is needed in younger patients, we will try to use the right and left mammary artery,” says Dr. Tong. “Exceptions are patients with coexisting obesity and diabetes, as this can make wound healing more difficult due to reduced blood flow to the sternum.” He adds that bilateral grafting can be considered in diabetics who are not obese and have good blood sugar control.
Use of the radial artery (RA) in bypass surgery was revived in the past decade after having been abandoned following high rates of graft occlusion. The renewed interest stems from new methods of preparation and drug treatment with antispasmodic agents to improve long-term results.
Advantages of RA grafts include easy preparation and availability for use in most patients. Also, because RA grafts involve arteries rather than veins, they are more resistant to development of atherosclerosis, a problem that plagues vein grafts. While medium-term results with RA grafts are good, these grafts’ long-term patency and outcomes are not yet fully known. RA grafts tend to work best when placed on an artery with a blockage of at least 70 percent — and preferably higher.
Advertisement
RA grafts are recommended for young patients when a third arterial graft is needed or when a patient requires two arterial grafts but the right ITA is unsuitable, Dr. Tong notes. They are also used in older patients more cautiously when alternative grafts are unavailable.
Because the RA has a relatively muscular wall, it has a tendency to go into spasm. If this artery is used as a graft, patients are placed on a calcium channel blocker for several months after surgery to keep the artery open.
Before RA graft use, an Allen test is performed to determine whether blood flow to the hand is sufficient. The artery can be harvested minimally invasively through a small incision. Wrist or hand numbness may occur as a side effect.
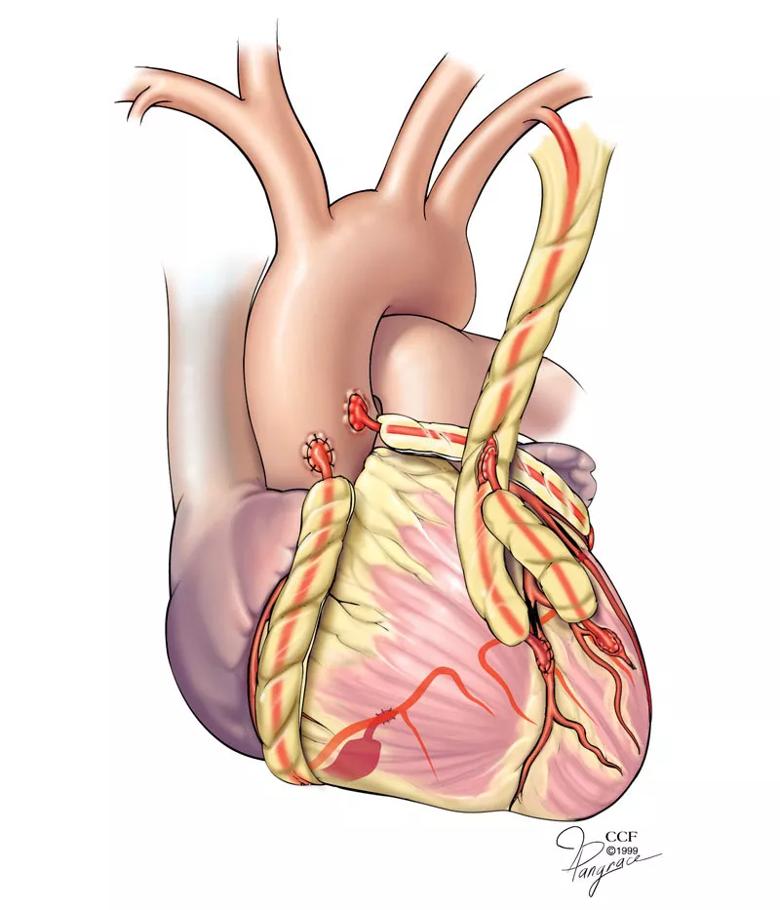
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/cbaa4f95-eb19-4bfd-9398-412af00a9dd3/15-HRT-3041-Artierial-Graft-CQD-Inset_jpg)
Illustration showing a few types of coronary artery bypass grafts: the free internal thoracic artery (lower left), the in situ internal thoracic artery (upper right) and the radial artery (middle right and center).
The gastroepiploic artery (GEA) has been used as a bypass graft usually to the right coronary artery. However, Dr. Tong notes that this rarely used graft type comes into play only if no other conduit is possible or when a fourth arterial graft is needed.
Bypass with a GEA graft is a technically difficult surgery to perform and is not a popular choice among surgeons. As it requires entering the patient’s abdomen, it is more invasive than other options but has a high likelihood of good long-term functioning when used in the right situation. In some patients a GEA graft represents an advantage over vein grafts.
Advertisement
The saphenous vein (SPV) is a commonly used conduit for bypass due to the ease of harvest, which can generally be done through minimally invasive procedures, with less scarring and faster recovery. But the failure of vein grafts over the long term remains a significant problem. Reasons for elevated failure rates include variable quality and size of the veins, the presence of valves within the veins and the potential for areas of dilatation (varicosities) within the veins. These and other factors can lead to flow pattern disturbances within the veins that can lead to early failure. The 10-year patency of vein grafts is approximately 60 percent, Dr. Tong observes.
“Many factors go into the choice of conduit used for bypass,” Dr. Tong concludes. “For older patients, an ITA graft and a vein graft will likely be suitable. For unstable sick patients or older patients, use of two or more arterial grafts may not be the best option because it requires longer and more tedious surgery. But if the patient is young and healthy and can tolerate a longer surgery, using multiple arterial grafts will give the best long-term result.”
Advertisement
Advertisement

A sampling of outcome and volume data from our Heart & Vascular Institute

Concomitant AF ablation and LAA occlusion strongly endorsed during elective heart surgery

Large retrospective study supports its addition to BAV repair toolbox at expert centers

Young age, solid tumor, high uptake on PET and KRAS mutation signal risk, suggest need for lobectomy

Surprise findings argue for caution about testosterone use in men at risk for fracture

Residual AR related to severe preoperative AR increases risk of progression, need for reoperation

Findings support emphasis on markers of frailty related to, but not dependent on, age

Provides option for patients previously deemed anatomically unsuitable