Locations:

Multifocal discharges need not rule out epilepsy surgery
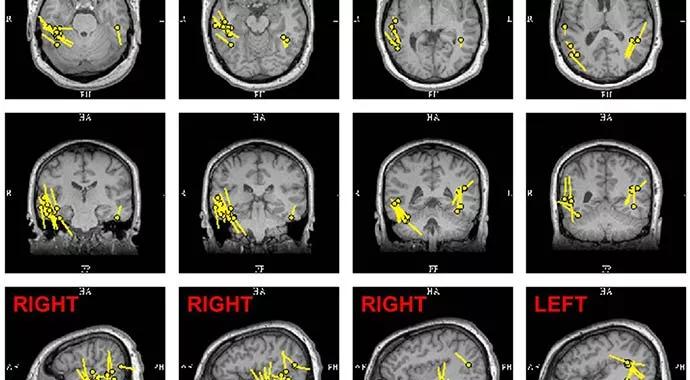
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/351aefc7-95c7-4298-b5d5-02b5af52f764/Case-Study-690x380_jpg)
Case-Study-690×380
By Juan Bulacio, MD, William Bingaman, MD, and Imad Najm, MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
The patient is a 24-year-old right-handed male college graduate who has had seizures since age 10 despite trials of more than eight antiepileptic medications. He reports two types of daily events (two to three per day):
Previous video EEG (VEEG) evaluations and imaging studies failed to localize the epilepsy. A noninvasive VEEG evaluation at Cleveland Clinic demonstrated frequent generalized and more rare left temporoparietal sharp waves and polyspikes. The patient’s habitual seizures were lateralized to the right hemisphere or nonlocalizable.
Review of brain MRI and voxel-based morphometric (VBM) analysis of the MRI suggested the presence of a right temporo-occipital malformation of cortical development (Figure 1).
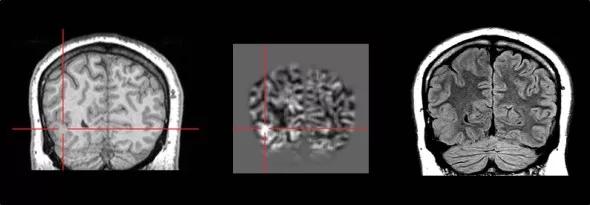
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/1872bae9-0388-468c-850b-246e8b735af8/Figure1a-e1440792606133_jpg)
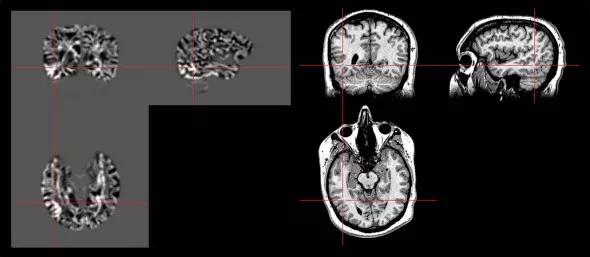
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/9eb461a0-fb88-4867-bdd6-b4a1320585ba/Figure1b-e1440792619151_jpg)
Figure 1, A (top) and B (bottom). Voxel-based morphometric (VBM) analysis of the MRI suggested the presence of a right temporo-occipital abnormality.
Subtraction single-photon emission computed tomography (SPECT) showed right posterior lateral temporal hyperperfusion extending to the inferior mesial occipital regions bilaterally (Figure 2). Magnetoelectroencephalography (MEG) recordings showed posterior temporal spikes on the right more than the left (Figure 3).
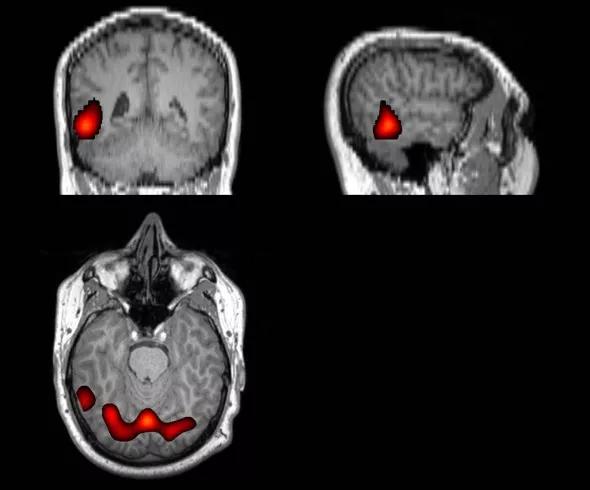
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/b8c1b448-a4fe-4bab-86ac-a8a4bfd82f12/Figure2-e1440792634393_jpg)
Figure 2. Subtraction SPECT images showed right posterior lateral temporal hyperperfusion extending to the inferior mesial occipital regions bilaterally.
Advertisement
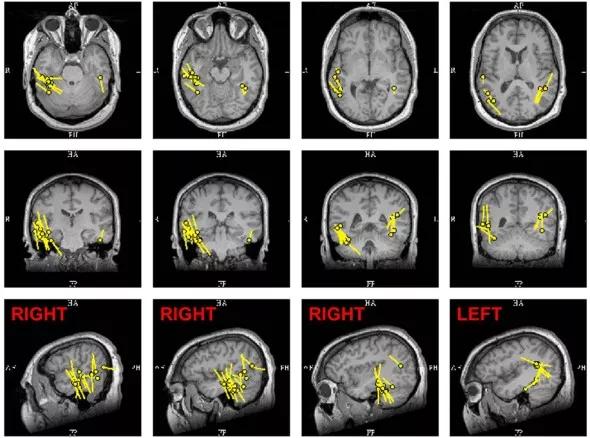
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/c970c07a-8438-4245-af8e-0bf29e2a5b8b/Figure3-e1440792646743_jpg)
Figure 3. MEG recordings showed posterior temporal spikes on the right more than left.
We recommended bilateral intracerebral electrode implantation in the temporoparieto-occipital regions (predominantly on the right) as part of a stereoelectroencephalographic (SEEG) evaluation to define the epileptogenic zone and understand the connections from this region. SEEG intracerebral electrodes were placed orthogonally lateral to mesial (Figure 4). Both interictal spikes and EEG seizure patterns were recorded from the basal/lateral temporo-occipital junction (electrodes D, Z, B and F). The epileptic regions were surrounding the MRI-identified lesion.
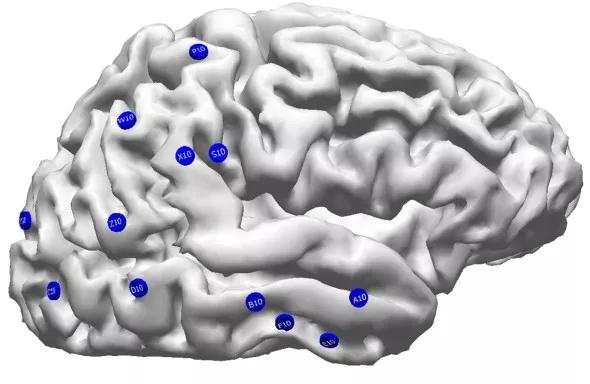
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/3ba8cbb1-6f7b-4ef2-ab4b-80e7f493a914/Figure4A-e1440792658207_jpg)
Figure 4A. SEEG depth electrodes on the right hemisphere.
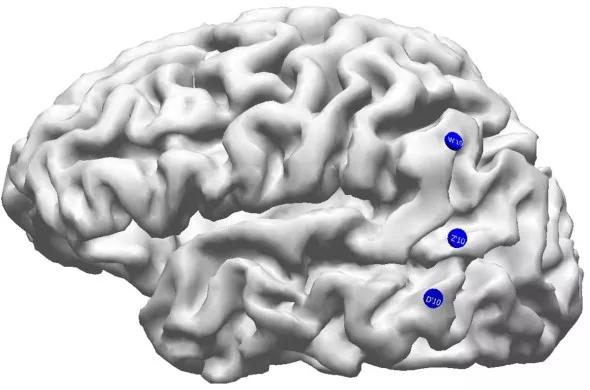
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/a1900a74-78be-4455-b75e-b3e793636f49/Figure4B-e1440792669118_jpg)
Figure 4B. SEEG depth electrodes on the left hemisphere.
The patient underwent a basal temporal resection guided by the SEEG results, the lesional anatomy and diffusion tensor mapping of the white matter to avoid the underlying geniculocalcarine tract.
The resected cortex was abnormal in texture and included the areas sampled by lateral contacts of electrodes D, Z, B and F. Considering the visual cortex was not primarily involved and there were no memory deficits and no epileptic hippocampal involvement, these two areas were spared. Pathology revealed mild focal cortical architectural disorganization in both horizontal and vertical orientations (focal cortical dysplasia type I).
The patient has been seizure-free since his surgery (eight weeks).
The best seizure outcome following epilepsy surgery is achieved in patients with an identifiable cortical lesion on MRI and concordant EEG and semiological features. For patients with no identifiable MRI lesion(s), or with an MRI lesion in the setting of discordant EEG and semiological features, further localization studies may be helpful in generating an anatomo-functional-clinical hypothesis that will guide SEEG intracerebral electrode implantation.
Advertisement
This case demonstrates that the presence of generalized and/or multifocal interictal epileptic discharges should not necessarily be a contraindication to epilepsy surgery. Bilateral/multifocal epileptic activities (so-called referred patterns) are more frequently found in patients with association cortex epilepsy. These findings may be due to the high network connectivity of the association regions with various areas of the brain bilaterally.
When it comes to the investigation of networks, SEEG represents a major advantage, given the possibilities it affords for bilateral exploration of homotopic regions of the brain in a three-dimensional view.
Wang ZI, Jones SE, Jaisani Z, Najm IM, Prayson RA, Burgess RC, Krishnan B, Ristic A, Wong CH, Bingaman W, Gonzalez-Martinez JA, Alexopoulos AV. Voxel-based morphometric magnetic resonance imaging (MRI) postprocessing in MRI-negative epilepsies. Ann Neurol. 2015;77(6):1060-1075.
Ristić AJ, Alexopoulos AV, So N, Wong C, Najm IM. Parietal lobe epilepsy: the great imitator among focal epilepsies. Epileptic Disord. 2012;14(1):22-31.
Gonzalez-Martinez J, Bulacio J, Alexopoulos A, Jehi L, Bingaman W, Najm I. Stereoelectroencephalography in “difficult to localize” refractory focal epilepsy: early experience from a North American epilepsy center. Epilepsia. 2013;54(2):323-330.
Dr. Bulacio is a staff physician in Cleveland Clinic’s Epilepsy Center.
Dr. Bingaman is Vice Chairman of Cleveland Clinic’s Neurological Institute and Head of the Section of Epilepsy Surgery in the Epilepsy Center.
Advertisement
Dr. Najm is Director of the Epilepsy Center.
Advertisement
Advertisement

New study advances understanding of patient-defined goals

Testing options and therapies are expanding for this poorly understood sleep disorder

Real-world claims data and tissue culture studies set the stage for randomized clinical testing

Digital subtraction angiography remains central to assessment of ‘benign’ PMSAH

Cleveland Clinic neuromuscular specialist shares insights on AI in his field and beyond

Findings challenge dogma that microglia are exclusively destructive regardless of location in brain

Neurology is especially well positioned for opportunities to enhance clinical care and medical training

New review distills insights from studies over the past decade