Locations:

How Cleveland Clinic supports one of its cardiovascular alliance partners

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/a4e507dd-25d0-452f-a765-09ebf5338cb7/MedStar-690x380_jpg)
MedStar-690×380
As detailed previously on Consult QD, Cleveland Clinic’s Miller Family Heart & Vascular Institute has built a network of affiliated and allied provider organizations across the U.S. to share best practices and help these organizations enhance their cardiovascular programs from clinical, operational and strategic perspectives. This post profiles how Cleveland Clinic’s relationship with one such partner organization, MedStar Heart & Vascular Institute, helped that organization improve one key aspect of its informatics operations.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Cleveland Clinic formed a clinical and research alliance in early 2013 with MedStar Heart & Vascular Institute, which serves a large population in the Maryland and Washington, D.C., region.
At the time, MedStar’s registry data collection process benefited from experienced cardiac surgery data abstractors and a solid IT infrastructure. However, there were multiple opportunities to align and integrate its two major repositories of registry information — for cardiac surgery and interventional cardiology — to provide more efficient, timely, accurate, validated, actionable and personal information to the clinical teams for quality process improvement.
To meet these challenges, MedStar leadership enlisted Cleveland Clinic’s support to create an integrated and centralized cardiovascular registry and quality process to accurately collect, validate, analyze and communicate results across the clinical disciplines and engage physicians in quality improvement initiatives. The broader aim was to provide a base for programmatic improvement and allow the health system to publish quality and outcome metrics to demonstrate overall service capabilities and value.
Beginning with its Washington Hospital Center, MedStar implemented the specific changes outlined below. At every step, its efforts were guided by administrative and clinical advisors from Cleveland Clinic, who shared processes and insights from their own experience with similar initiatives at Cleveland Clinic.
Advertisement
MedStar has seen some early successes in the wake of these changes, including a substantial decline in risk-adjusted mortality after aortic valve replacement (Figure 1) and a marked increase in use of the radial artery for PCI procedures (Figure 2), which decreases bleeding complications, reduces length of stay and increases patient satisfaction.
Additional outcomes of the initiative include:
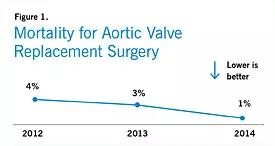
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/8e9d1572-2844-4995-a544-d555e2f26040/MedStar-Fig1-sm-e1441921235719_jpg)
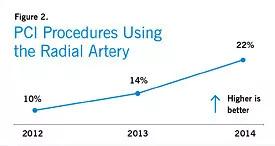
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/4032c10e-169b-440f-b994-a4bbd20b1c10/MedStar-Fig2-sm-e1441921267358_jpg)
“Partnering with Cleveland Clinic has given us the opportunity to focus our physicians and staff on fostering a transparent, outcomes-based environment while also allowing us to benchmark ourselves against the best heart program in the world,” says Allen Taylor, MD, Chief, Division of Cardiology, MedStar Heart & Vascular Institute. “To help us get there, they shared best practices around implementation of a high-quality data and informatics program, which enabled us to obtain clean data that we could act on. And the ongoing collaboration on developing a pathway to performance transformation provides tremendous value to our organization.”
Advertisement
Advertisement

A sampling of outcome and volume data from our Heart & Vascular Institute

Concomitant AF ablation and LAA occlusion strongly endorsed during elective heart surgery

Large retrospective study supports its addition to BAV repair toolbox at expert centers

Young age, solid tumor, high uptake on PET and KRAS mutation signal risk, suggest need for lobectomy

Surprise findings argue for caution about testosterone use in men at risk for fracture

Residual AR related to severe preoperative AR increases risk of progression, need for reoperation

Findings support emphasis on markers of frailty related to, but not dependent on, age

Provides option for patients previously deemed anatomically unsuitable