Locations:

Expert insights on managing HCM when debulking isn’t an option
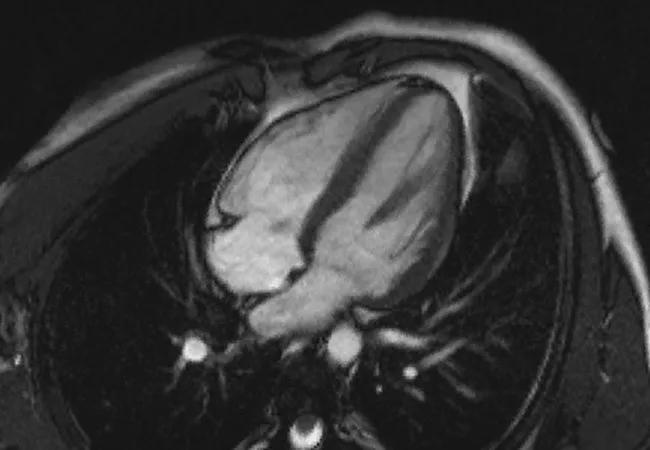
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/84204a3a-b1af-4475-af03-c6f26d3c0737/HCM_jpg)
Multimodal imaging is drawing back the septal curtain in cases of HCM without wall thickness
Bulk is a defining characteristic of hypertrophic cardiomyopathy (HCM). A thick heart is a dysfunctional heart. But an increasing number of patients are being identified as having all the dysfunction with little or none of the thickness. How can this be? And how do you treat these patients when the best strategy, debulking, is no longer an option? Cleveland Clinic specialists are collaborating on the answers to these questions, and in the process they’re opening up a new world of knowledge about HCM in all its manifestations.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“Imaging is the key to our understanding of HCM,” says cardiologist Milind Desai, MD, Professor of Medicine at Cleveland Clinic Lerner College of Medicine, “and echocardiography is the mainstay of diagnosis.”
Echocardiography confirms that about 70 percent of patients with HCM have left ventricular outflow tract obstruction (LVOTO). In most cases, LVOTO is largely responsible for the symptoms of HCM — i.e., dyspnea, fatigue, chest pain, syncope, etc. — thus explaining the alternate nomenclature hypertrophic obstructive cardiomyopathy (HOCM).
Dr. Desai recently led a Cleveland Clinic study (Circ Cardiovasc Imaging. 2015;8:e003132) that sought to understand LVOTO in 121 patients with HCM without thick walls. The retrospective study used advanced echocardiography and a newer modality, cardiac magnetic resonance (CMR), to quantify the features of mitral valve and papillary muscle abnormalities in patients with HCM and then confirm whether these abnormalities could be responsible for LVOTO in these patients.
Using these data, Dr. Desai and co-authors substantiated the independent effect of three factors:
“We used the strengths of each modality,” explains Dr. Desai. “Echocardiography was useful in the delineation of highly mobile mitral valve leaflets, while CMR allowed us to characterize papillary muscle morphology and apical displacement, and to quantify systolic mobility.”
Advertisement
Building on previous reports, this study is the largest analysis of HCM without severe septal hypertrophy published to date.
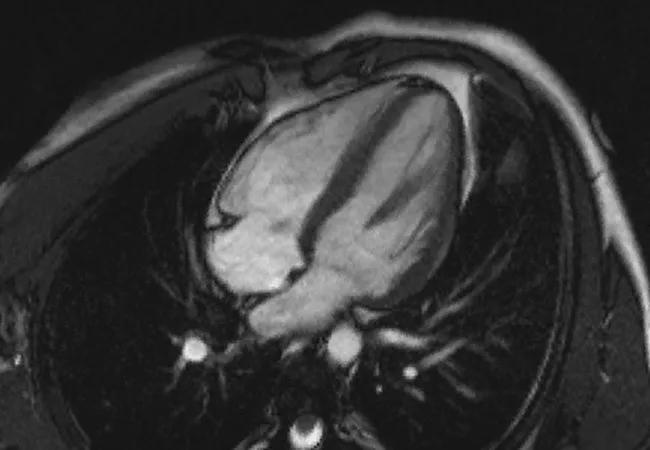
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/84204a3a-b1af-4475-af03-c6f26d3c0737/HCM_jpg)
MRI of a patient with severe obstruction but minimal septal hypertrophy.
“The idea that there could be obstruction without thick walls is relatively new — it’s only been around about six or seven years,” observes study co-author Harry Lever, MD, a cardiologist in Cleveland Clinic’s Section of Cardiovascular Imaging. “The mechanism is to be found in the dynamic interplay among the mitral valve leaflets, chordae and papillary muscles.”
A key factor is the anterior mitral valve leaflet, which was found to be abnormally long in many of the patients studied. The long leaflet buckles toward the septum during systolic contraction. This obstructs the left ventricular outflow tract. Another factor is a structural anomaly known as bifid papillary muscle. Excessive mobility of the bifid papillary muscle distorts the movement of the mitral leaflet during systole. These factors, along with anomalies of the chordae, all contribute to LVOTO.
Refractory HCM is traditionally addressed through a septal myectomy, which restores normal systole dynamics and provides almost immediate relief of symptoms. Cleveland Clinic surgeons have performed more than 3,000 septal myectomies over the past 50 years, including 207 in 2016. And mortality for the procedure at Cleveland Clinic is consistently well below the expected rate, coming in at approximately 0.2 percent over the past 10 years. Alcohol ablation, which may take weeks to relieve symptoms, is used to shrink the septal wall in patients who are not eligible for myectomy.
Advertisement
Neither of these alternatives will help patients who have severe obstruction with thin walls. In the absence of better choices, patients are often offered mitral valve replacement alone or with a light myectomy. Valve replacement resolves some LVOTO issues but is considered less than ideal for what is generally a younger patient population that should be spared the rigors of lifelong anticoagulation.
Using the knowledge quantified in the study led by Dr. Desai, Cleveland Clinic has developed a multidisciplinary approach to the treatment of thin-wall HCM. Cardiovascular surgeon Nicholas Smedira, MD, Professor of Surgery at Cleveland Clinic Lerner College of Medicine and a co-author of the study, works with colleagues like Drs. Lever and Desai to develop treatment strategies for patients with thin-wall LVOTO.
“Mitral valve replacement is to be avoided,” says Dr. Smedira. “If the problem is the length of the anterior mitral valve leaflet, we can go in and shorten it. This reduces contact with the septum during systole, and spares the native valve.”
In patients in whom bifid papillary muscle mobility is the larger issue, Dr. Smedira surgically reorients the papillary muscles away from the septum.
Dr. Lever describes these techniques as “plastic surgery for the heart.”
The study by Dr. Desai and colleagues goes a long way toward drawing back the septal curtain that obscures the independent factors contributing to LVOTO. Through use of multimodality imaging, it has produced a more nuanced picture of HCM — and lays the groundwork for future progress.
Advertisement
“Our findings strengthen our commitment to personalizing treatment for HCM — and to ensuring that every patient gets the most appropriate treatment for his or her condition,” says Dr. Desai. “Advanced echocardiography combined with CMR provides a rich core of data to help us make treatment decisions that are in the patient’s best interest.”
Advertisement
Advertisement

A sampling of outcome and volume data from our Heart & Vascular Institute

Concomitant AF ablation and LAA occlusion strongly endorsed during elective heart surgery

Large retrospective study supports its addition to BAV repair toolbox at expert centers

Young age, solid tumor, high uptake on PET and KRAS mutation signal risk, suggest need for lobectomy

Surprise findings argue for caution about testosterone use in men at risk for fracture

Residual AR related to severe preoperative AR increases risk of progression, need for reoperation

Findings support emphasis on markers of frailty related to, but not dependent on, age

Provides option for patients previously deemed anatomically unsuitable