Locations:

How MRI postprocessing can enable surgery in “nonlesional” cases
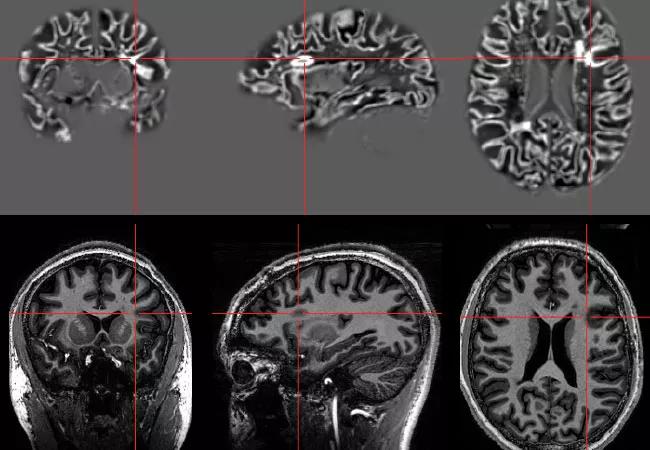
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/f8480fc5-6a92-4833-a4e1-5d3979e0add1/16-NEU-2599-Wang-650x450_jpg)
16-neu-2599-wang-650×450
By Irene Wang, PhD; Stephen Jones, MD, PhD; Elaine Wyllie, MD; Imad Najm, MD; and Jorge Gonzalez-Martinez, MD, PhD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
At 18 years of age, “Randy” (not his real name) was being evaluated for the second time for possible epilepsy surgery. At age 12, he had undergone extensive testing at another center, but results were complicated. MRI was interpreted as normal, EEG and clinical features indicated left frontal lobe epilepsy, and invasive recording with subdural electrodes indicated that the seizure onset zone was overlapping with language function. When counseled that resective surgery would result in a speech deficit, the family declined to proceed.
Over the years since his seizures had begun at age 5, Randy tried many antiepileptic medications, without relief. His seizures increased, occurring at rates from one or two per month up to 20 per day. He and his family wanted a second look at surgery, and came to Cleveland Clinic’s Epilepsy Center for further consultation.
Randy again underwent standard presurgical testing to localize the site of seizure onset, including MRI, PET, ictal SPECT and MEG. He also participated in a research protocol, established and approved by Cleveland Clinic’s institutional review board since 2014, that allowed him to have a 7T MRI for comparison with the standard 3T MRI obtained in clinical practice.
Results from the 7T MRI were impactful: With greatly enhanced resolution and detail, the research MRI revealed a subtle but clear malformation of cortical development in the depth of the left inferior frontal sulcus, with thickened cortex and indistinct gray-white junction as shown in Figure 1.
Advertisement
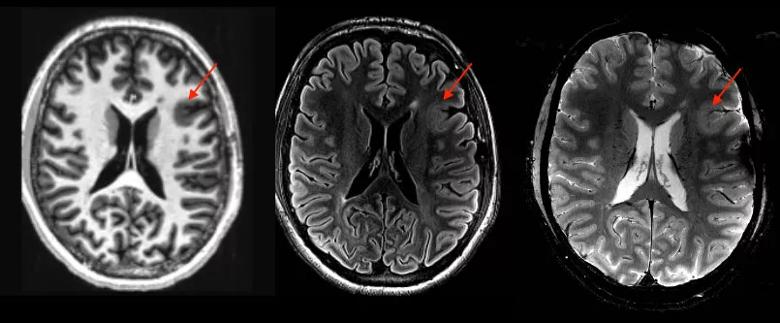
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/e361d4b7-45f6-42b5-a847-666d56f41839/16-NEU-2599-Wang-Inset1_jpg)
Figure 1. 7T MRI identified a focal malformation of cortical development located at the depth of the left inferior frontal sulcus (arrows). Left: T1-weighted MP2RAGE sequence. Middle: T2 FLAIR sequence. Right: R2*-GRE sequence.
This lesion was confirmed by postprocessing of the 7T MRI using a quantitative voxel-based morphometry approach,1 as shown in Figure 2. In retrospect, the lesion was also visible on Randy’s 3T MRI, although with less conspicuity.
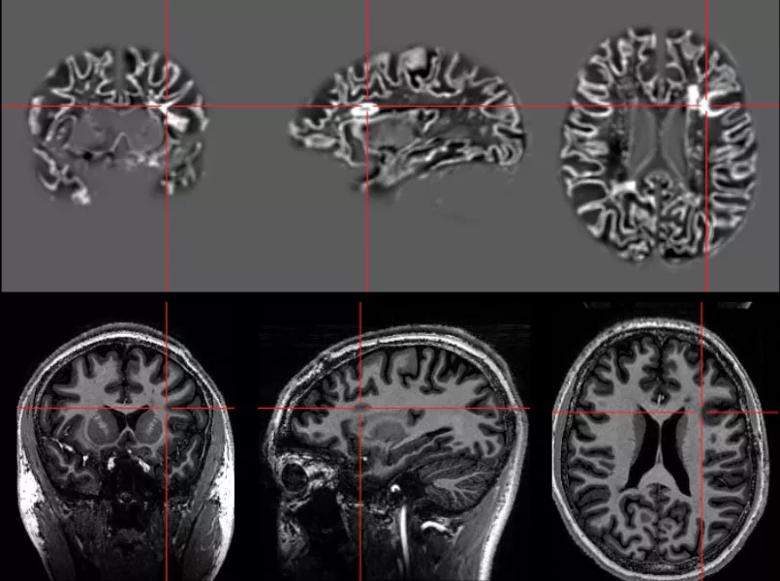
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/c1259c70-fa3a-4352-8b66-79285db39d2f/16-NEU-2599-Wang-Inset2_jpg)
Figure 2. Postprocessing of the 7T MRI using a quantitative voxel-based morphometry approach confirmed the lesion location, shown here by crosshairs.
Results from video-EEG, PET, MEG and ictal SPECT (Figure 3) also showed convergent findings suggesting that seizures were arising from the region of the malformation in the depth of the left inferior frontal sulcus.
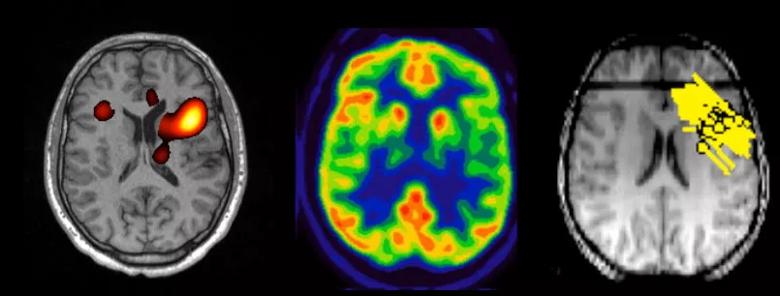
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/2c7d411b-b61f-43f4-90a0-88ce06869637/16-NEU-2599-Wang-Inset3_jpg)
Figure 3. Three different imaging modalities — ictal SPECT (left), interictal FDG-PET (middle) and interictal MEG (right) — showing concordant localization with lesion location.
Thanks to the cutting-edge neuroimaging, Randy’s lesion was visualized for surgical planning. The remaining concern was its proximity to the usual location of Broca’s area, the inferior frontal region critical for speech production. After intense multidisciplinary discussion, Epilepsy Center physicians designed a combination evaluation with stereotactic depth and subdural electrodes to (1) confirm seizure onset from the region of the lesion seen on MRI, (2) map the location of Broca’s area and (3) develop a strategy for language-sparing resection.
Advertisement
Meticulous analysis of the invasive evaluation revealed evidence of high epileptogenicity restricted to the dysplastic cortex in the depth of the left inferior frontal sulcus (Figure 4, left). The surface cortex surrounding the abnormal sulcus was secondarily involved as the seizures evolved.
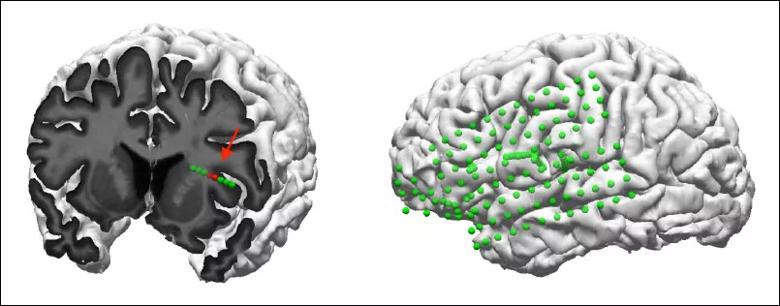
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/27b4e8d9-1690-4dac-8eee-9d20d2df7aa7/16-NEU-2599-Wang-Inset4_jpg)
Figure 4. (Left) Cortical rendering of the patient’s MRI with coronal cut plane showing the implanted depth electrode traversing the MRI lesion (arrow). The red contacts indicate where ictal onset was seen. (Right) Image showing implantation coverage via superimposition of the three subdural grids and four depth electrodes on the brain surface.
As shown in Figure 5, functional speech cortex was mapped on surface cortex posterior to abnormal sulcus that was not primarily epileptogenic, delineating a resective surgical approach expected to be both effective and safe.
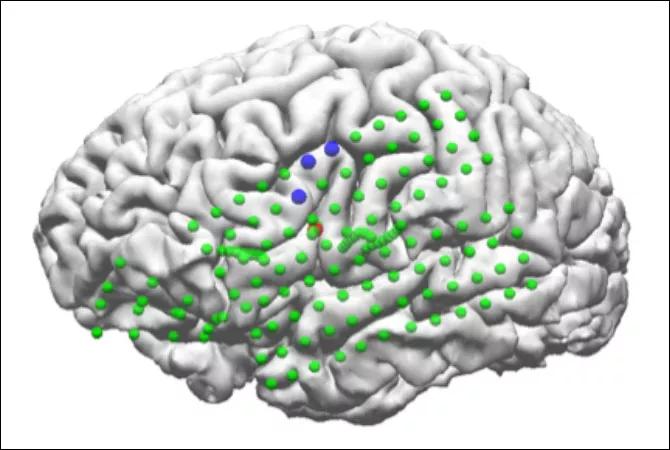
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/a047eba1-d6fc-4ecb-8ba1-4b25b67cdaa4/16-NEU-2599-Wang-Inset5_jpg)
Figure 5. Image showing the spatial relationship between lesion (red contacts, deep in the brain) and language function (blue contact on brain surface).
Based on all these evaluations, Randy underwent focal resection of the lesion with intraoperative electrocorticography guidance under awake conditions. Language function was intact postoperatively, and the active intraoperative electrocorticograph normalized after the resection, showing absence of pathological patterns.
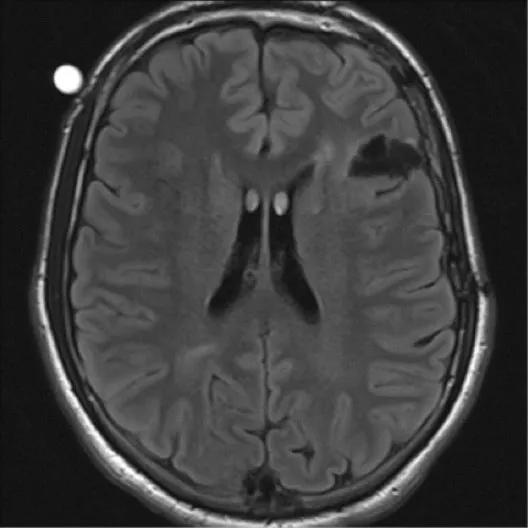
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/418a207b-d4d6-45ba-9b1a-e091cbc5f306/16-NEU-2599-Wang-Inset6_jpg)
Figure 6. Postoperative MRI showing the left inferior frontal resection, including the MRI-visible area of cortical malformation.
Four months after surgery, he had a single cluster of five seizures on one day, with he no further seizures after medication adjustment. While long-term follow-up is needed to judge the full effect of surgery, his epilepsy appears to have been positively impacted.
Advertisement
Randy’s case illustrates the benefits of advanced neuroimaging with 7T MRI and postprocessing. By enhancing the lesion characteristics and rendering them more easily detectable, these techniques led to precise implantation of depth and subdural electrodes and then a strategy for surgery.
In contrast, the “nonlesional” MRI prior to his first surgical evaluation led to implantation only of subdural electrodes on the cortical surface, which captured the exit patterns but not the origins of seizure discharges emanating from the deep lesions. Since these spread patterns overlapped with language cortex, the opportunity for surgery was obscured.
By exploring and exposing increasingly subtle focal malformations of cortical development, advanced neuroimaging may allow more patients to benefit from epilepsy surgery than ever before.
Dr. Wang is a staff scientist in Cleveland Clinic’s Epilepsy Center
Dr. Jones is Vice Chairman for Research and Academic Affairs of Cleveland Clinic’s Imaging Institute.
Dr. Wyllie is a pediatric epileptologist in Cleveland Clinic’s Epilepsy Center and Professor in the Cleveland Clinic Lerner College of Medicine.
Dr. Najm is Director of Cleveland Clinic’s Epilepsy Center.
Dr. Gonzalez-Martinez is a neurosurgeon in Cleveland Clinic’s Epilepsy Center.
Advertisement
Advertisement

New study advances understanding of patient-defined goals

Testing options and therapies are expanding for this poorly understood sleep disorder

Real-world claims data and tissue culture studies set the stage for randomized clinical testing

Digital subtraction angiography remains central to assessment of ‘benign’ PMSAH

Cleveland Clinic neuromuscular specialist shares insights on AI in his field and beyond

Findings challenge dogma that microglia are exclusively destructive regardless of location in brain

Neurology is especially well positioned for opportunities to enhance clinical care and medical training

New review distills insights from studies over the past decade