Locations:

Patient referred to Lupus Clinic with array of symptoms

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/1b0ea303-9d83-497e-8b6f-da0985f78972/Smith-Hojjati-Hero-Image-690x380pxl_jpg)
Smith-Hojjati-Hero-Image-690x380pxl
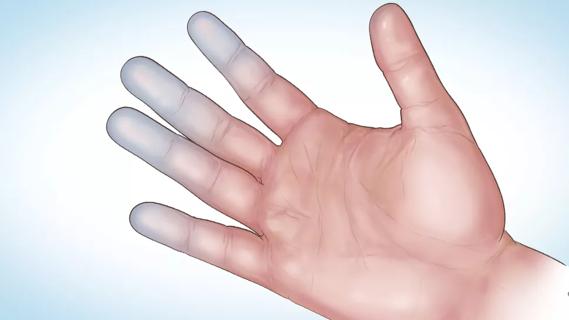
A 29-year-old woman presented to her primary care physician reporting six weeks of swelling of the fingers and knees, facial rash, and stabbing pain in the chest with breathing. Examination confirmed pleurisy and edema (Figure 1), and lab results revealed anemia, leukopenia and positive ANA findings.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/4d325145-443b-481a-a367-9f1dab9338aa/Smith-Hojjati-Inset-Image-590pxl-width_jpg)
Figure 1. Radiograph showing pleural and pericardial effusion in the case patient.
She was referred to Cleveland Clinic’s Lupus Clinic for further evaluation and treatment, where she was diagnosed with SLE and found to also have pericarditis and proteinuria. She was started on oral steroid therapy and further evaluated by subspecialists in cardiology, nephrology and dermatology. Additional testing was conducted, including a kidney biopsy.
Her physicians conferred with the referring physician, and a coordinated course of therapy was proposed. It was decided to initiate treatment with the IV immunosuppressants cyclophosphamide and methylprednisolone followed by oral hydroxychloroquine, prednisone and mycophenolate mofetil. The patient received detailed education about her disease and the proposed treatment. After her questions and concerns were addressed, treatment started. She fared well, with rapid resolution of the arthritis, rash and pericarditis. Her kidney function improved, and six months later she had only mild proteinuria and mild renal insufficiency.
Advertisement
Advertisement
Treatment strategies require understanding of pathomechanisms

Education, prevention strategies and monitoring serves this at-risk group

Treatment for scleroderma can sometimes cause esophageal symptoms

Lupus Clinic providers collaborate to advance treatment and understanding

Older Psoriasis Patients May Experience Quicker Transition

Cleveland Clinic’s Rheumatic Lung Disease program treats patients with complex conditions

Symptoms complement one another

E-coaching program is tailored for those with the disease