Locations:

Component shift can occur without loosening
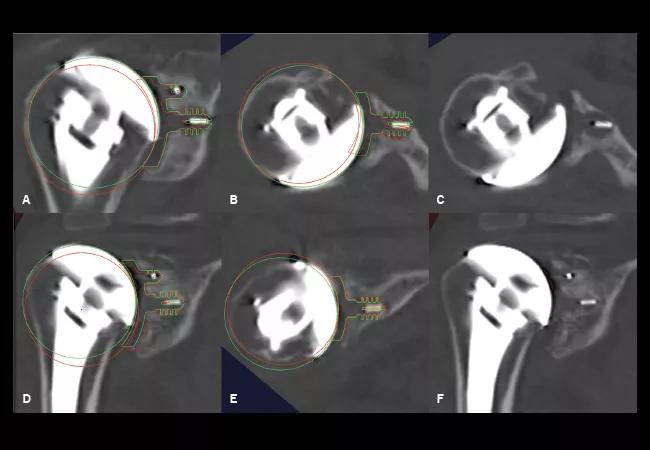
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/12c9e457-5789-4987-ae5c-4857b6a9616f/16-ORT-2560-Hero-Image-650x450pxl_jpg)
16-ORT-2560-Hero-Image-650x450pxl
By Eric Ricchetti, MD; Bong-Jae Jun, PhD; Thomas Patterson, PhD; and Joseph Iannotti, MD, PhD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
One of the most common complications following total shoulder arthroplasty (TSA) is glenoid component loosening. Yet routine imaging can be insufficient to predict when loosening will occur and to determine a precise and accurate component position over time. To solve this problem, we tested whether using 3-D computed tomography (CT) analysis would identify changes in glenoid component position over time that standard imaging methods cannot detect.
We enrolled 41 patients who had undergone TSA with a polyethylene anchor peg glenoid component for sequential CT scanning and analysis. Each enrollee had a preoperative study (CT1), an early postoperative study within three months of surgery (CT2), and a postoperative study performed at a minimum of two years after surgery (CT3) (see figure). They also had routine plain radiographs and Penn Shoulder Scores at the two-year follow-up visit.
We performed the postoperative CTs using metal artifact reduction techniques. We used a custom 3-D image analysis software to detect the location of the glenoid and humeral head components based on four metal markers embedded in the pegs of the glenoid component and a volumetric center fit to the humeral head component. This technique allowed us to determine glenoid component version, inclination and joint line position. It also allowed us to determine humeral head alignment.
We measured humeral-glenoid alignment and humeral-scapular alignment in the anteroposterior and superoinferior dimensions based on the relationship of the center of the humeral head to the glenoid and scapular planes, respectively. On the postoperative CT scans, we also assessed backside seating of the glenoid component and presence of peg radiolucencies, including evidence of osteolysis versus bone integration of the central anchor peg. We compared those CT scans to findings on plain radiographs.
Advertisement
We found that 27 percent of patients (11 of 41) showed evidence of glenoid component shift, which we defined as a change in component position of 5 degrees or more in version and/or inclination from CT2 to CT3. Importantly, the patients’ plain radiographs showed no obvious evidence of component shift, and patients with and without component shift did not have significantly different Penn Shoulder Scores.
Advertisement
Our findings demonstrate that glenoid component shift can occur without obvious implant loosening at short-term follow-up and suggest that component deformation or bone remodeling may occur over time. Improved backside seating of the glenoid component can also occur over time in stable implants due to bone remodeling. While radiostereometric analysis studies have shown evidence of component shift over time, they cannot be used to assess for bony integration of the implant. We believe follow-up investigations using larger patient cohorts are needed to clarify our findings and determine their long-term clinical impact.
Dr. Ricchetti is staff in the Department of Orthopaedic Surgery. Drs. Jun and Patterson are researchers in the department. Dr. Iannotti is Chair of the Orthopaedic & Rheumatologic Institute.
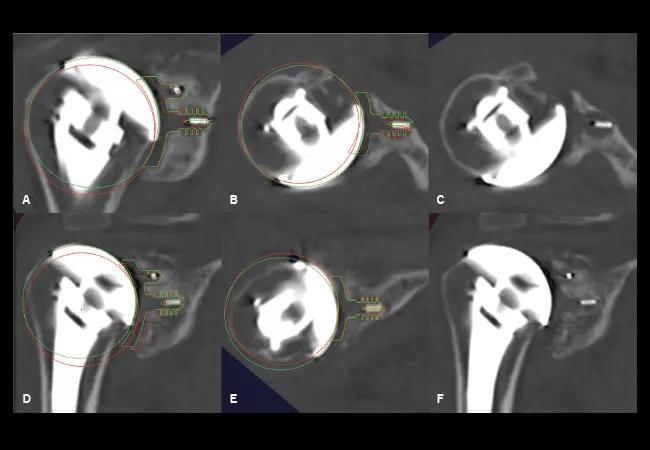
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/c1ecbfaa-4ea7-4d5f-9890-7a5802541592/16-ORT-2560-Inset-Image-650pxl-width_jpg)
Figure: Digital templates of the position of the glenoid and humeral head components on the immediate postoperative CT (red) and two-year follow-up CT (green) are superimposed on the two-year follow-up CT in two patients (A-C, D-F). In the first patient (A-C), the glenoid component has shifted into increased inclination (A) and retroversion (B), and central anchor peg osteolysis is seen on the two-year follow-up CT after the digital templates are removed (C). In the second patient (D-F), the glenoid component has shifted into increased inclination (D) with stable version (E), and bone integration around the central anchor peg is seen on the two-year follow-up CT after the digital templates are removed (F).
Advertisement
Advertisement
Advertisement

Biologic approaches, growing implants and more

Study reports zero infections in nearly 300 patients

How to diagnose and treat crystalline arthropathy after knee replacement

Study finds that fracture and infection are rare

Center will coordinate, interpret and archive imaging data for all multicenter trials conducted by the foundation’s Osteoarthritis Clinical Trial Network

Reduced narcotic use is the latest on the list of robotic surgery advantages

Cleveland Clinic specialists offer annual refresher on upper extremity fundamentals

Cleveland Clinic orthopaedic surgeons share their best tips, most challenging cases and biggest misperceptions